As I explained last month in part 1, during the randomization process, we generate and allocate interventions to trial arms in a way that ensures that neither the investigators nor the participants know or can predict ahead of time what treatment the patients will receive. Simple, restricted block, and stratified randomization methods have been presented so far, and now minimization will be explained. Minimization is a randomization method that ensures balance of important prognostic factors between treatment groups without the disadvantages of stratification.
Minimization, a form of restricted randomization, is considered to be a dynamic method, since the randomization list is not produced before the trial starts, but during participant recruitment. Additionally, minimization, in contrast to the previous methods, is considered to be an adaptive randomization technique, since future participant allocation depends on previous assignments.
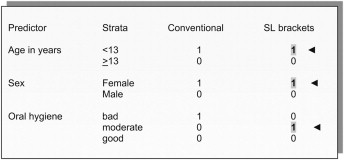
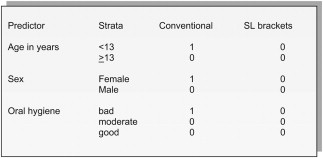
In the trial example assessing the periodontal condition of orthodontic patients fitted with either conventional or self-ligating appliances, randomization by using the minimization method can assign participants to groups and use 3 prognostic factors: age (<13 or >13 years), sex (male or female), and oral hygiene status before treatment (bad, moderate, or good). The first patient or the first few patients are assigned through simple randomization (like tossing a coin). Let us assume that the first patient was assigned by using simple randomization to the conventional group and has the following characteristics: less than 13 years old, female, and bad oral hygiene ( Fig 1 ). The patient is entered 3 times, which is equal to the number of the prognostic factors that we seek to balance for. The second patient will be assigned to the arm that improves the balance according to the preselected set of prognostic factors between the 2 trial arms. The second patient arrives and has the following characteristics: 11 years old, female, and moderate oral hygiene ( Fig 2 ).
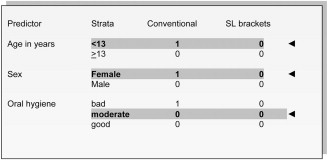
The next step is to calculate the marginal totals (marginal totals = sum of counts per treatment arm) at the line indicated by the arrows in each treatment arm for the prognostic factors of the second patient; the objective is to balance the marginal totals of the prognostic factors. On the conventional appliance treatment arm, the sum of the counts for patients enrolled who are younger than 13 years and female, and have moderate oral hygiene is 1 + 1 + 0 = 2; for the self-ligating appliance arm, the marginal total is 0 + 0 + 0 = 0.
Therefore, to improve the balance of age, sex, and oral hygiene status, the second patient must be randomized into the self-ligating appliance arm; the allocation of this patient is shown in Figure 3 .