Score
0
1
2
Gold standard assessment
Sound, no evidence of demineralization
Demineralization extending into enamel only
Demineralization extending into enamel and outer dentin
CAMBRA based recommendations
Assess/address
Assess/address risk factors
Assess/address risk factors
Risk factors
Arrest/remin early lesion with therapeutics
Treat with minimal intervention (e.g. sealant or small restoration)
3.3 Caries Detection Methods
Caries on fissured surfaces account for over 80 % of all caries on young permanent teeth [26]. Dental radiography may not effectively identify early non-cavitated lesions on critical tooth surfaces. Occlusal caries continue to be difficult to identify and monitor, particularly in the early stages, using conventional methodologies. The nature of dental decay, especially pits and fissure caries, has changed dramatically with the use of fluoride, where lesions are often hidden underneath an intact veneer of surface enamel [27]. Therefore, in many cases, occlusal lesions develop slowly and do not cavitate, making lesion detection with conventional methods even more challenging than in the past. The hidden nature of occlusal caries makes diagnosis very subjective with visual inspection, where staining of the fissures can increase false positives and lead to unnecessary treatment. For occlusal lesions, tactile and visual inspection have been shown to have low sensitivity, ~0.3, because of the hidden nature of the lesions [28]. Tactile and visual inspection offer high specificity ~0.95 for advanced occlusal lesions that extend into the dentin, but the specificity is below 0.80 for lesions confined to the enamel that can be treated with non- surgical therapy [29]. The ability to detect near cavitated lesions is in itself problematic because the insertion of a sharp explorer can advance the progression of a lesion by damaging the outer surface of the lesion [30] and cause ingress of bacteria. Since conventional use of tactile assessment using a sharp explorer is no longer the gold standard for a clinical exam, teledentistry has potential to provide an evaluation close to the standard of care, with the exception of using tactile methods to feel the surface zone of smooth surface lesions [31]; however, these lesions are likely to be managed with topical therapies until obvious cavitation.
Optical caries detection systems have the potential to assist with visual assessment for the use of teledentistry. The list of systems on the market at the time of this article is extensive and expanding. Optical caries detection can be categorized as either scattering-based or fluorescence-based. The aim of this chapter is to not review all of these systems but highlight studies that are the most relevant to oral health evaluation in teledentistry. Most of these studies focused on assessing permanent teeth rather than primary teeth.
3.4 Scattering-Based Optical Scattering Detection Systems
Newer optical methods, such as the Midwest Caries ID™ (MID) and CP-OCT, have the potential to detect early non-cavitated occlusal lesions using non-ionizing, safe radiation (light). Increasing the accuracy of detecting and assessing early carious lesions with either objective direct measurements or an imaging modality that can allow remote assessment would serve children in critical communities. A potential objective caries detection measurement that could be collected by adjunct personnel may be accomplished using readings from the visible light based Midwest Caries ID™ (Dentsply, York, PA) [32–34]. There is potential for adjunct personnel to electronically send a table of recorded readings from Midwest Caries ID™ to aid an offsite dentist in treatment planning.
Another emerging method for teledentistry includes near infrared imaging modalities, such as Cross-Polarization Optical Coherence Tomography (CP-OCT) [35, 36]. CP-OCT can be compared conceptually to ultrasound imaging since both techniques use an incident beam and measure a reflected or backscattered signal. Conventional OCT and the polarized enhanced CP-OCT has been shown to detect early carious lesions through an increase in light scattering [37–39]. CP-OCT is promising because it performs a real time optical image of the microstructure of the tissue, without radiation or surgical intervention [40]. Multiple OCT images can be produced within seconds, which is advantageous as a clinical detection technique [37]. The rapid acquisition of CP-OCT imaging can allow adjunct dental personnel to use the device for preventive dental screenings. Acquired CP-OCT images can later be interpreted by a dentist; however, there are few comparisons between other less costly optical devices, such as the Midwest Caries ID™ (MID) and simple visual camera images (CAM).
The MID uses a Light-Emitting Diode to emit a range of red light and then measures the scattering of light due to mineral changes experienced from carious lesions to determine if carious lesions exist [33, 34]. Red light normally scatters in sound tissue in a predominantly forward direction with minimal light being backscattered. As the mineral content of the measured area becomes less mineralized, more back scattering is detected, since demineralization causes isotropic (360°) scattering [41]. MID detects this increase in backscattering but there are few studies examining how much backscattering intensity is interpreted as caries. The individual measurements with the MID device occurred after calibration of the device. Teeth should be kept moist. The tip of the device can be inserted vertically on the surface of each tooth and moved around slightly (without pressure) in the pits and fissure area between the reference points. The MID uses a red indicator light to communicate to the examiner the presence of demineralization. In addition the MID produces sound at two frequencies; with the higher frequency designed to detect higher scattering being associated with a larger more extensive amount of decay (score = 2).
Both CP-OCT and MID (Fig. 3.1) do not have markedly superior diagnostic values from simple CAM assessment when assessing non-cavitated lesions (Table 3.2). These values were calculated from a gold standard of histology examination after sectioning [15]. It is important to keep in mind that, ICDAS-II score 1 and 2 teeth have both been shown to have demineralization extending into the dentin in approximately 17–33 % of in vitro cases [19, 42, 43]. Although MID and CP-OCT were useful in detecting the presence of demineralization, examiners were not able to utilize these devices to adequately assess the depth of the demineralization. The limitations of CP-OCT can be explained when examining Fig. 3.1. Demineralization caused the incident linearly polarized NIR light to be highly scattered and depolarized. The pit and fissure area near the reference point ‘r1’ (Fig. 3.2b, arrow) indicated extensive demineralization for E5 and E6 that was much greater than small surface demineralization; however, the scattering was so extensive in the upper portion of the lesion that the full extent of the demineralization was not measured by CP-OCT. This was likely because the scattering degraded and attenuated the incident light. The CP-OCT NIR light could not penetrate deep enough through the entire lesion. This observation agrees with past studies where demineralization in enamel hides the underlying tooth structure [44, 45]. It is important to point out that although the intensity of the incident light and the sensitivity of the CP-OCT detector can be increased in the future, improving these factors may not be able to markedly improve signal penetration, especially at intensity levels that are safe for diagnostic CP-OCT imaging.
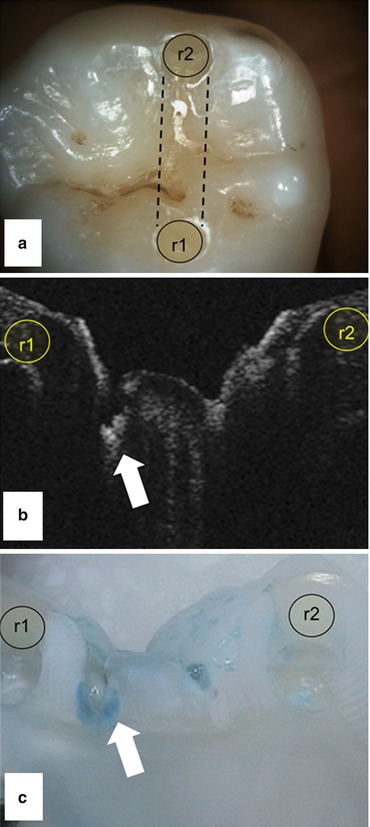
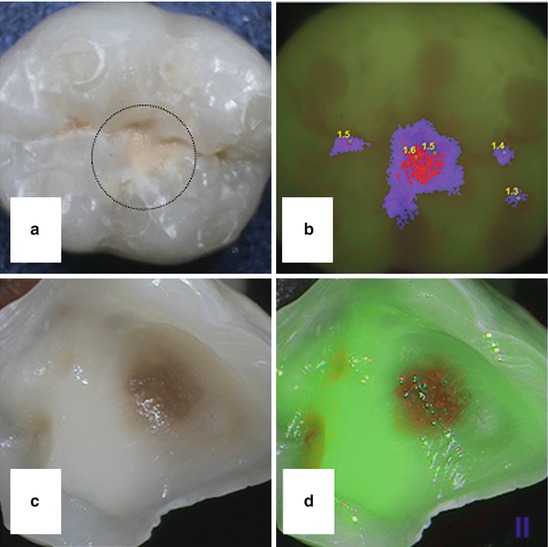
Fig. 3.1
Each tooth had two composite reference points (r1 and r2). The test area was the fissure area between the points. (a) All CAM images were assessed Score ‘2’. All MID Scorings were ‘0’. (b) CP-OCT images were taken before tooth sectioning. CP-OCT images are presented in grayscale. Black areas have low scattering and white areas have high scattering. All CP-OCT scorings were ‘2’ based on the fissure area near r1 (arrow). (c) Histological evaluation using caries indicator dye confirmed demineralization extending into enamel and dentin with Score of ‘2’(arrow) (Picture from Van Hilsen et al., BMC Oral Health, 2012)
Table 3.2
Comparison between visual camera (CAM) based caries assessment and scattering based caries detection methods: Midwest Caries ID (MID) and CP-OCT
|
Disease defined as score 1, 2
|
Disease defined as score 2
|
ICC (95 % CI)
|
|||
|---|---|---|---|---|---|
|
Sen
|
Sp
|
Sen
|
Sp
|
||
|
CAM
|
80.5
|
52.5
|
48.0
|
57.8
|
0.75 (0.64–0.84)
|
|
MID
|
46.9
|
85.0
|
17.3
|
88.0
|
0.83 (0.75–0.90)
|
|
CP-OCT
|
83.4
|
45.0
|
44.2
|
72.7
|
0.49 (0.34–0.65)
|
Fig. 3.2
(a) Visual image (CAM) of an extracted tooth with a lesion that did not penetrate past the DEJ (Teledentistry lesion score = 1). (b) The fluorescence–based imaging (Spectra/VistaProof®) illuminates the tooth with 405 nm light and quantifies the degree of fluorescence emitted with a false color scale. (c) Perioperative images of a tooth after the majority of dentinal caries were removed. Stained dentin remained. (d) Fluorescence–based imaging (Soprolife®) illuminates the tooth with 450 nm light and the green and red shifted fluorescence is visualized. The red shift fluorescence correlates strongly with the visual brown staining seen in (c). All analysis was done soon after extraction to preserve porphyrins concentration within the tooth (Images from author)
Another limitation in CP-OCT imaging was that it was difficult to assess the fissure depth in reference to the DEJ. The DEJ was not apparent in the majority of the images of this study. This was likely caused from the internal reflection angle (critical angle) of light traveling through enamel back to the detector. To clarify, as the returning (back-scattered) signal traveled back through the enamel toward the tooth surface, the signal could be internally reflected when the occlusal topography angles were greater than 37–54° to incident plane (the range is dependent on the water moisture level). In certain occlusal samples, internal reflection could attenuate the backscattered signal from deeper enamel and dentin layers from returning to the CP-OCT for measurement. Another explanation is that the CP-OCT system could not actively focus well below the surface to acquire the deeper DEJ signal; however, the low numerical aperture lens on the probe was designed to capture deeper signals.
To assess examiner agreement and reliability when assessing sound versus any demineralization (score 0 versus 1, 2), the Intraclass Correlation Coefficient (ICC) was calculated for each of these methods (Table 3.2). This ICC value represents an agreement of four readings: two examiners each making two separate assessments spaced 1–2 weeks apart. MID was found to have the highest ICC, and the overall CP-OCT ICC indicated that there was high variability in assessing the images. This highlights an important and often overlooked assessment of caries detection used in teledentistry. Reliability in caries assessment is crucial, and CP-OCT requires a highly skilled and trained evaluator.
3.5 Fluorescence-Based Optical Detection Systems
Fluorescence-based detection systems have been extensively studied and used in clinical practice. Common examples are the Diagnodent® (KaVo Dental, Lake Zurich, IL, USA), the Soprolife® intraoral fluorescence camera (Acteon, La Ciotat, France), the VistaProof® intraoral fluorescence camera (Dürr Dental, Bietigheim-Bissingen, Germany) which is marketed in the U.S. as the Spectra®
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


