Introduction
Microcomputed tomography offers a unique opportunity to accurately examine orthodontically induced inflammatory root resorption. The aims of this study were to quantify, in 3 dimensions, the amount of root resorption caused by placing heavy and light distal root tipping forces on premolars and to compare the prevalence of root resorption in different areas of the tooth.
Methods
Thirty maxillary first premolars from 15 patients who were to have these teeth extracted as part of their orthodontic treatment were selected for this study. Each tooth in the same patient was randomly chosen to have either a 2.5° or a 15° distal root tipping bend placed for 4 weeks. After the experimental period, the teeth were extracted according to a strict protocol to prevent damage to the root. They were then imaged by a microcomputed tomography scan x-ray system (SkyScan 1172, SkyScan, Aartselaar, Belgium) and analyzed by software designed for volumetric measurements.
Results
A significant difference was found in the amount of total root resorption between light and heavy forces ( P = .021). The mean cube root volumes of the resorption craters in the 15° tip-bend group were greater than in the 2.5° tip-bend group. This significance was lost when the tooth was divided into vertical thirds, although a trend was still present. When the areas of expected compression in the periodontal ligament were compared with the areas of expected tension, significance was seen in the apical and cervical thirds only.
Conclusions
Based on this experiment, one can conclude that a 15° distal root tip bend causes more orthodontically induced inflammatory root resorption than a 2.5° distal root tip bend. Furthermore, greater root resorption was found in areas under pressure when compared with areas under tension.
Orthodontically induced inflammatory root resorption (OIIRR), a particular type of external root resorption, is an inevitable consequence of orthodontic tooth movement. Root resorption has been described as a physiologic or pathologic process that results in a loss of substance from mineralized cementum and dentin. After the application of an orthodontic force, the periodontal ligament becomes compressed, leading to areas of local inflammation and aseptic necrosis that is histologically called hyalinization. Elimination of this hyalinized tissue is carried out by an invasion of cells and blood vessels from the adjacent undamaged periodontium. This results in alveolar bone resorption, allowing orthodontic tooth movement to occur; however, it also leads to removal of tooth structure. Resorption has been noted not only in teeth that have received orthodontic treatment, but also in untreated teeth, suggesting that it is a normal, physiologic process. The range of incidences and freq-uencies of OIIRR seen in the literature partly reflects the various methodologies and techniques used to study it.
If OIIRR enters dentin, it is irreversible, and if it becomes extensive, it can compromise the outcome of orthodontic treatment. Although this level of severity is rare, it is important that one recognizes and understands the risk factors, pathogenesis, and preventive factors involved. Risk factors might be either biologic, which can be difficult to modify because they are intrinsic to the patient, or mechanical. Mechanical risk factors that have been identified include the duration of treatment ; the duration, direction, and magnitude of force application; and the distance of tooth movement.
Traditionally, OIIRR has been investigated from a quantitative point of view by using radiographs such as orthopantographs and periapical films. This method has the advantages of simplicity, low radiation dose, and the ability to be used in vivo. Nevertheless, this technique has a major limitation, since root resorption is a 3-dimensional phenomenon, and plain radiographs can only evaluate in 2 dimensions. Other techniques that have been used include light microscopy, scanning electron microscopy, and conventional computed tomography, all of which have problems of accuracy, practicality, or radiation dosage. It would appear, however, that the highest accuracy for quantifying the volume of root resorption craters is with 3-dimensional techniques such as scanning electron microscopy and microcomputed tomography. The most significant disadvantage of these techniques is that they need to be used on extracted teeth; this makes them impractical after extended orthodontic treatment.
Force magnitude and OIIRR are of interest to clinicians, since emphasis has been placed on the importance and supposed benefits of light forces in orthodontics. Many animal and human studies have confirmed that the amount of root resorption is proportional to the orthodontic force, with only a few studies contradicting this. Volumetric studies with the more accurate microcomputed tomography technique have found more resorption with greater forces.
The aim of this study was to analyze the volume of resorption craters with microcomputed tomography after the application of 2.5° and 15° of distal root tipping bends on premolars. This study is a continuation of the root resorption investigations carried out by the orthodontic department of the Faculty of Dentistry at the University of Sydney in Australia.
Material and methods
The sample consisted of 30 maxillary first premolars from 15 patients (11 girls, 4 boys) who required removal of these teeth as part of their planned orthodontic treatment. Due to differences in bone density between the mandible and the maxilla, only maxillary teeth were used. The mean age of these patients was 14 years 2 months, with a range of 12 years 8 months to 16 years 11 months. The selection criteria for this study were (1) no previous reported or observed dental treatment to the teeth to be extracted, (2) no previous reported or observed trauma treatment to the teeth to be extracted, (3) no previous reported or observed orthodontic treatment involving the teeth to be extracted, (4) no past or present signs or symptoms of periodontal disease, (5) no past or present signs or symptoms of bruxism, (6) no significant medical history that would affect the dentition, (7) no physical abnormality in the anatomy of the craniofacial or dentoalveolar complex, (8) completed apexification, and (9) residence in a region with nonfluoridated water.
Furthermore, the patients were instructed not to take any nonsteroidal anti-inflammatory drugs or similar drugs during the experimental period. Each subject’s left or right side was randomly selected to receive either a 2.5° or a 15° distal tipping force. Ethics approvals were obtained from the University of Ondokuz Mayis in Turkey (2008/346) and the Central Sydney Area Health Service Ethics Review Committee (10-2008/11235).
SPEED orthodontic brackets with a 0.022-in slot (Strite Industries, Cambridge, Ontario, Canada), were bonded to the maxillary first molar, second premolar, and first premolar. A 0.017 × 0.025-in beta-titanium molybdenum alloy wire was used to create the distal tipping force on the first premolar. Either this wire was bent or the excess composite under the bracket was used to ensure passivity.
The first molars in the opposing arch of all patients were bonded with a layer of Multi-cure glass ionomer cement (3M Unitek, Monrovia, Calif). This cement served 2 purposes: to open the occlusion to reduce occlusal interferences on the study premolars, and to minimize appliance damage ( Fig 1 ).
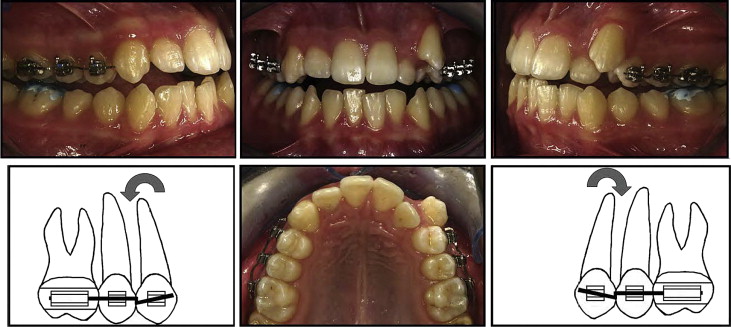
This passive wire was then removed, and a bend was placed so that it applied the desired amount of distal root tip (2.5° or 15°). A template was used to standardize the tipping degrees, and a 2.5° additional tip was added to overcome the play between the 0.22-in slot bracket and the 0.017 × 0.025-in beta-titanium molybdenum alloy wire. This wire was inserted and left in place for 4 weeks without reactivation ( Fig 1 ).
One operator (T.T.) treated all patients during this phase. After the 4-week experimental period, the teeth were extracted by 1 of 2 oral surgeons, who adhered to a strict method previously established to minimize damage to the cementum. The teeth were then placed in individual containers of deionized water (Milli-Q, Millipor, Bedford, Mass), which has been described as an appropriate storage medium. Any residual periodontal ligament and soft tissue were removed in an ultrasonic bath for 10 minutes, and then the tooth was rubbed with damp gauze. Next, the teeth were immersed in 70% alcohol for 30 minutes for disinfection and replaced into the Milli-Q water. The teeth were bench dried for at least 48 hours before analysis, which was carried out by a desktop microcomputed tomography x-ray system (SkyScan 1172, Aartselaar, Belgium). The protocol, software, and equipment used to quantify root resorption crater volumes were the same as described in a previous study. By using engineering principles, the moments theoretically applied at the brackets with 2.5° and 15° of distal root tipping bends were calculated to be 3.58 and 54.87 Nm, respectively (written communication by Li Q., Senior Lecturer in Biomedical Engineering, School of Aerospace, Mechanical and Mechatronic Engineering, The University of Sydney, Sydney, 2009).
Results
Three-dimensional images of each tooth were saved. As described previously, each crater was isolated and recorded with known x-, y-, and z-coordinates. Statistical analysis was carried out by using univariate analysis of variance (ANOVA) with the Statistical Package for the Social Sciences (version 16 for Windows; SPSS, Chicago, Ill). The cube root of the volumetric readings was taken to create an appropriate model for the statistical analysis. The volumes were combined to create an equivalent hemispheric crater, and the radii of these craters for each tooth were compared. This method has been used in previous studies. The fixed factor was the force, the random factor was the subject, with the amount of resorption as the response.
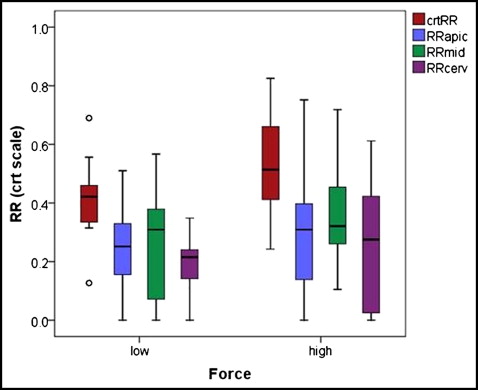
The ANOVA model showed a significant difference in the amount of total root resorption between light and heavy forces ( P = 0.021), with the mean cube root volumes of the resorption craters in the 15° tip-bend group approximately 1.3 times greater than in the 2.5° tip-bend group ( Table I , Fig 2 ). Although the trend remained, this significance was lost when the individual vertical thirds ( Fig 3 , A ) of each tooth were considered (apical third, P = 0.399; middle third, P = 0.202; cervical third, P = 0.281). Age and sex had no effect in this sample ( P = 0.128 and P = 0.283, respectively).
| Location on tooth | Estimated means for cube root volume | P value | ||
|---|---|---|---|---|
| 2.5° tip bend | 15° tip bend | SE | ||
| Overall | 0.411 | 0.528 | 0.032 | 0.021 |
| Apical third | 0.254 | 0.309 | 0.045 | 0.399 |
| Middle third | 0.267 | 0.354 | 0.046 | 0.202 |
| Cervical third | 0.195 | 0.256 | 0.039 | 0.281 |
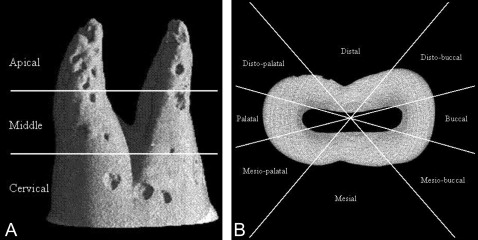
Hypotheses were tested for resorption in certain areas. Each tooth was divided into mesial, mesiobuccal, buccal, distobuccal, distal, distopalatal, palatal, and mesiopalatal segments ( Fig 3 , B ) and also into vertical thirds. The amount of resorption in particular sectors was compared to that in others. For example, there were greater amounts of root resorption between the distobuccal, distal, and distopalatal sectors compared with the mesiobuccal, mesial, and mesiopalatal sectors in the apical third ( P = 0.001) ( Table II ). Furthermore, greater amounts of resorption were observed in the distobuccal, distal, and distopalatal sectors of the middle third, but this difference was marginally significant at P = 0.057. Conversely, there was significantly more resorption in the mesiobuccal, mesial, and mesiopalatal sectors compared with the distobuccal, distal, and distopalatal sectors in the cervical third ( P = 0.002).
| Vertical third | Compression-tension | Paired differences | P value | ||
|---|---|---|---|---|---|
| Mean ∗ | SD | SE mean | |||
| Apical | DP + D + DB-MP + M + MB | 0.1573038 | 0.2352623 | 0.0429528 | 0.001 |
| Middle | DP + D + DB-MP + M + MB | 0.0929597 | 0.2568812 | 0.0468999 | 0.057 |
| Cervical | MP + M + MB-DP + D + DB | 0.1166297 | 0.1822461 | 0.0332734 | 0.002 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


