Phase 2 Therapy Periodontal Surgery—Corrective Phase
Summaries
Periodontal surgical therapy is only one component of complete periodontal treatment. If surgery is necessary, it is usually performed as a second phase (corrective), following a thorough evaluation of the clinical results of Phase 1 therapy. The patient must be motivated, and must exhibit adequate plaque control. The first phase of initial therapy, professional supragingival tooth cleaning, must be complete. In addition, clinical studies have demonstrated that the debridement of subgingival calculus and biofilm must be performed before surgical intervention. Following such extensive pre-treatment, surgery is less often necessary, the surgical procedures are associated with less hemorrhage, and the morphological results are better, with less tissue loss (“longer teeth” are less of a problem).
The primary goal of periodontal surgery is strictly antiinfective, meaning that the surgical modality aims to eliminate infection of pockets that have not responded to conservative treatment and/or medicinal adjuncts. Surgical intervention is therefore indicated with deep pockets, intraosseous defects and furcation involvements.
The secondary goal is the correction of defects in cases of unphysiologic gingival and osseous architecture, with special regard to creation of conditions that simplify or guarantee efficient plaque control, especially in the interdental areas.
Pocket depth reduction and/or pocket elimination maintain their importance in contemporary periodontal therapy (Slots 2002, Petersilka et al. 2002, Socransky & Haffajee 2002).
Toward these goals, a vast array of various surgical techniques is available; they will be described.
The following important aspects will be considered:
-
Purposes and goals of periodontal surgery
-
Patient selection and defect factors
-
Influences on the treatment results
-
Periodontal surgery: methods and indications
-
Furcation problems, defects and classifications
-
Furcation treatment
Purposes and Goals of Periodontal Surgery
Periodontal surgery, its goals and purposes, can only be considered in conjunction with complete periodontal treatment. For example, initial therapy and surgery are two entities with identical goals, but which use different methods to achieve these goals (closed root planing versus root planing with direct vision). Furthermore, initial therapy may be the only therapy required for mild periodontitis, whereas in severe cases it may represent only a preparatory presurgical phase.
The goals often cannot be achieved using a single specific surgical procedure; rather, often combinations of various surgical methods are required, either simultaneously or one following upon the other:
-
Root cleaning/debridement with direct vision
-
Reduction or elimination of plaque-retentive areas that promote infection, especially periodontal pockets
-
Elimination of inflammation
-
Enhancing the regeneration of periodontal tissues
-
Elimination of diseased tissues—resective therapy
-
Creation of physiologic morphology/architecture of the marginal periodontium
-
Correction of mucogingival defects, restoration of esthetics in the aveolodental tissues
Root Cleaning with Direct Vision (Access Flap)
The root surfaces are exposed to clinical view either by reflecting a gingival flap or, less often, following excision of the gingiva (gingivectomy, p. 301). Plaque and calculus can then be removed from all root surfaces, including furcations, irregularities etc., with direct vision.
Removal of Infection-enhancing Niches
The most important niche for subgingival microbial flora are periodontal pockets themselves. Also of importance are open furcations, root irregularities, fusions, grooves and other oral structures.
Periodontal pockets can be eliminated by flap surgery or gingivectomy (resective therapy). One may also attempt to heal the defects, especially bony pockets, through regenerative surgical procedures (pp. 299, 301).
The above-mentioned root irregularities, fusions and grooves can be reduced by means of careful odontoplasty, usually after flap reflection.
Elimination of Inflammation
The clinical procedures described above (root debridement or planing and reduction of niches) lead to the elimination of the causes of periodontal inflammation. Clinical symptoms of activity such as exudation, bleeding and suppuration are eliminated. Freedom from inflammation always leads to consolidation of the gingival tissues, shrinkage or gingival recession; this alone results in a more or less pronounced pocket depth reduction.
Enhancing Regeneration of Periodontal Tissues
The hoped for results of surgical procedures include not only cessation of the disease process, but also “healing” of the pocket via regeneration of periodontal tissues.
This goal has been approached with some successes during the past two decades. The implantation of bone and bone replacement materials into the intraalveolar pockets, the GTR technique, the use of matrix proteins and in the future, use of growth factors are extremely promising. Unfortunately, the predictability of success using these methods is, today, neither understood nor reliable (see also patient factors, p. 297).
Elimination of Diseased Tissues—Resective Therapy
As mentioned above, the results of regenerative surgical procedures cannot always be predicted with certainty. But the practitioner strives for a “pocket free” periodontium whenever possible, especially when restorative/reconstructive procedures are planned upon those teeth that were previously periodontally involved.
Investigations by the Slots group (Tuan et al. 2000) have also demonstrated that following resective procedures (osseous surgery), in comparison to simple “access flap” procedures, the depth of the residual pockets is less, and also the colonization by periodontopathic microorganisms (anaerobic!) is more significantly reduced following use of more radical surgical procedures.
Creation of Physiologic Morphology of the Marginal Periodontium
During the course of periodontitis within any given patient, gingival swelling or on the other hand gingival shrinkage may occur. Therefore, the goal of surgical intervention is to create a harmonic course of the gingival margin, which is achieved through the choice of incision (sulcular, paramarginal), the recontouring of the alveolar bone and the type of flap repositioning, usually at a somewhat more apical niveau. In addition to improved esthetics, plaque control should also be simplified for the patient.
Correction of Mucogingival Defects—Re-Creation of Esthetics
The purposes and goals of mucogingival surgery include the widening of the attached gingiva, which is usually associated with deepening the oral vestibulum. Another major goal is soft tissue coverage in areas of gingival recession and correction of alveolar ridge defects, which anticipate additional treatment in the areas of prosthetics and dental implantology.
Patient Selection
In most industrialized nations today, every patient has the “right” to medical/dental treatment.
The term “selection” therefore does not imply ruling out any type of therapy; treatment recommendations and the definitive treatment plan may vary considerably for each individual patient. The general medical history, local and systemic risk factors, “behaviors,” understanding of the individual oral situation and the interdependent consideration of the patient’s compliance are critical.
Perhaps most important, even beyond the active treatment itself, are follow-up examinations (and treatments) during recall appointments. The long-term success of periodontitis treatment must be secured life-long, and this is a demand that not every patient can fulfill.
All of these factors lead to the obvious conclusion that the therapeutic possibilities and the type of therapy may be quite different for each individual patient. These possibilities may range from a purely palliative treatment with a severely reduced prognosis, to systematic and synoptic periodontitis therapy including surgical procedures, functional therapy, comprehensive reconstructions and even dental implants.
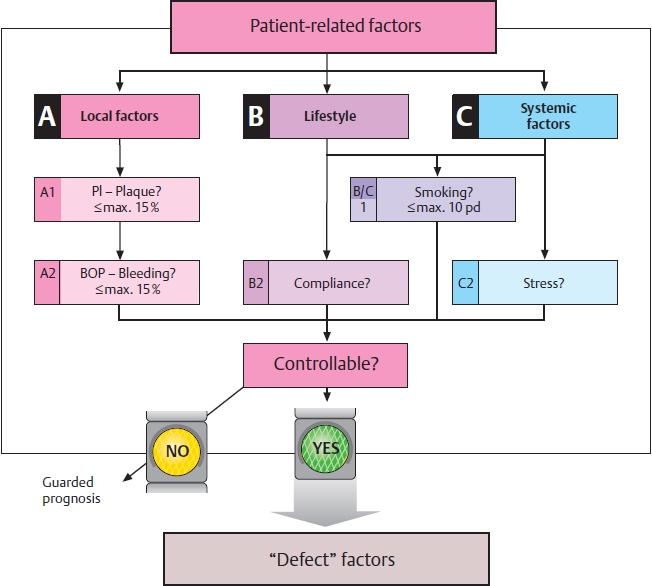
Defect Factors
In addition to the listed patient factors, there are, of course, also defect factors such as morphologic defects, that are of importance for the prognosis of any therapeutic procedure. Included here are the width and thickness of the gingiva (phenotype), course of the horizontal bone loss and the depth of supra-alveolar pockets. Most importantly:
-
Intra-alveolar defects are classified as 1-, 2- or 3-wall bony pockets, with consideration of the depth and the width of the “opening angle” of the defect, acknowledging that most of these defects represent “combined” bony pockets: In the apical region, three walls are in evidence, in the “middle,” two walls, and coronally only one wall!
-
Furcation involvement, and its severity
-
In patients with gingival recession, the depth and width of the gingival recession (Miller classification, p. 162) is of importance for predicting the therapeutic success.
Both patient factors and local defect factors—as well as the “aptitude” of the clinician, are of determining significance for the planning, type of surgical procedure and the ultimate results (see next page).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


