Geminated teeth occur more frequently in the deciduous dentition than in the permanent dentition, with prevalence figures of 0.6% and 0.1%, respectively. Bilateral presentation is rare. A survey of the literature showed that the prevalence estimates for bilateral double teeth range from 0.01% to 0.04% in the deciduous dentition, and 0.05% in the permanent dentition. In this article, we report a rare case of bilateral fusion of the maxillary permanent incisors, discuss possible histogenetic mechanisms related to this anomaly, and explain the treatment management.
Dental anomalies of forms can occur in the deciduous and permanent dentitions. Various terms have been used to describe dental twinning anomalies. “Double teeth,” “double formations,” “joined teeth,” “fused teeth,” “synodontia,” “schizodontia,” “concrescence,” and “dental twinning” are often used to describe fusion or gemination.
The phenomenon of gemination arises when 2 teeth develop from 1 tooth bud, and, as a result, the patient has a larger tooth but a normal number, in contrast to fusion, when the patient appears to be missing a tooth, if the double tooth is counted as 1 unit. In geminated teeth, division is usually incomplete and results in a large tooth crown with a single root and a single canal. Fused teeth arise through the union of 2 normally separated tooth germs, and, depending on the stage of tooth development at the time of union, they can be either complete or incomplete. However, fusion can also be the union of a normal tooth bud to a supernumerary tooth germ. In these cases, the number of teeth is also normal, and differentiation from gemination might be difficult, if not impossible. Supernumerary teeth are not uncommon, and they appear in 0.3% to 3.8% of the population. Double teeth originate from the morpho-differentiation stage of tooth development; however, the exact etiology is unclear. Pressure or a physical force producing close contact between 2 developing tooth buds has been reported as a possible cause. Evolution, trauma, and genetic and environmental factors have also been implicated as contributing factors. Double teeth might also be part of syndromes such as achondrodysplasia, chondroectodermal dysplasia, and KBG (the name of the syndrome is based on the initials of the first three patients reported by Hermann in 1975). In contrast to other dental anomalies, double teeth occur more frequently in the deciduous dentition than in the permanent dentition, with prevalence figures of 0.6% and 0.1%, respectively, in white patients. They are found predominantly in the anterior region, with incisors and canines the most frequently affected. Geminated teeth are usually found in the maxilla, but cases of fusion are more frequently found in the mandible. Bilateral presentation is rare, as reported by Duncan and Helpin. A survey of the literature showed prevalence estimates for bilateral double teeth ranging from 0.01% to 0.04% in the primary dentition, and 0.05% in the permanent dentition.
In this article, we report a rare case of bilateral fusion of the maxillary permanent incisors and discuss the possible histogenetic mechanisms related to this anomaly and the treatment options for the patient.
The esthetic and functional implications of bilateral fusion usually require complex restorative, periodontal, surgical, and orthodontic treatments, and a multidisciplinary approach is needed. Hemisection can be considered an appropriate treatment alternative for a permanent tooth fused with a supernumerary tooth.
Case report
The patient, a 12-year-old white girl, was referred by her dentist because of the morphologic abnormality of 2 teeth. The patient’s main complaints concerning her teeth were their unesthetic appearance. The clinical intraoral examination showed double teeth (maxillary central incisors). No supernumerary teeth were observed, and all permanent teeth were present.
She came for an orthodontic consultation with a Class I malocclusion, a symmetrically proportionate face, and a concave profile ( Fig 1 ). Intraoral and dental cast examinations ( Figs 2 and 3 ) indicated a maxillary left central incisor that was rotated distopalatally, and oversized maxillary right central incisor (14 mm mesiodistally) and maxillary left central incisor (16 mm). The remaining permanent teeth were of normal size and shape. Overbite was 1 mm, and overjet was 2 mm. Each of the 2 central incisors had an incisal notch in the central part of the incisal edge. Both teeth responded positively to electrical pulp testing. The radiographs showed 2 distinct roots of the left and right central incisors ( Fig 4 ), and their pulp chambers were individualized. No periapical radiolucency was associated with these teeth, since the lamina dura were intact. All remaining permanent teeth in each arch were fully erupted and of normal size and morphology.


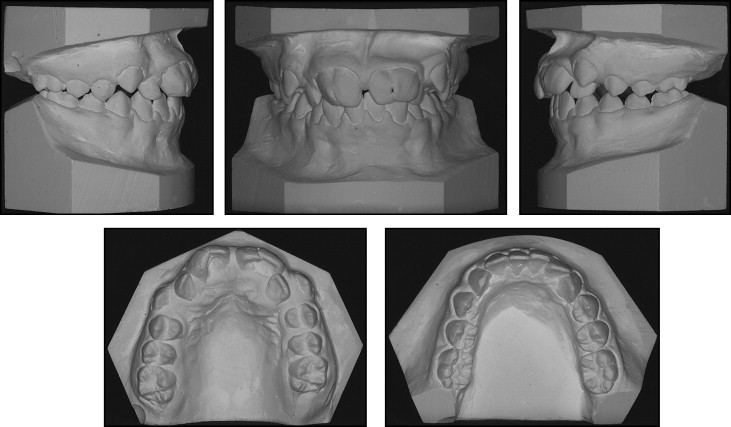

The patient had a dental Class I malocclusion, with crowding in both arches and the maxillary left lateral incisor in crossbite ( Fig 3 ). Her medical history was uneventful.
After dental sectioning ( Figs 4, 5 , and 6 ), the 2 mesial fused fragments of the crown roots were extracted under local anesthesia and separated longitudinally throughout the root conjunction line.



