The orofacial muscle is an important factor in the harmony of the occlusion, and its dysfunction significantly influences a patient’s occlusion after craniofacial growth and development. In this case report, we describe the successful orthodontic treatment of a patient with unilateral orofacial muscle dysfunction. A boy, 10 years 0 months of age, with a chief complaint of anterior open bite, was diagnosed with a Class III malocclusion with facial musculoskeletal asymmetry. His maxillomandibular relationships were unstable, and he was unable to lift the right corner of his mouth upon smiling because of weak right orofacial muscles. A satisfactory occlusion and a balanced smile were achieved after orthodontic treatment combined with orofacial myofunctional therapy, including muscle exercises. An acceptable occlusion and facial proportion were maintained after a 2-year retention period. These results suggest that orthodontic treatment with orofacial myofunctional therapy is an effective option for a patient with orofacial muscle dysfunction.
Highlights
- •
An adolescent boy had an anterior open bite and weak facial muscle force.
- •
Orthodontic treatment was combined with orofacial myofunctional therapy.
- •
Acceptable occlusion and facial proportion were achieved and maintained for 2 years.
The harmonization between the teeth and the orofacial muscles is an important factor in an adequate occlusion, and suitable occlusal forces have been reported to play a significant role in keeping the teeth in balance. This stabilizing effect was evident in a patient who could not squeeze his teeth together: the absence of occlusal forces allowed the teeth to extrude and tip, and to be generally unmanageable.
The masticatory muscles influence craniofacial growth and development. Strong muscles form the face, whereas the facial form in persons with weak muscles is more varied because the muscles exert less influence. Some studies have shown morphologic improvements in children with open bites who practice chewing exercises. Therefore, facial exercises are useful, to some extent, in reversing the adverse effects of a lack of adequate orofacial muscle force on facial skeletal growth.
Orofacial myofunctional therapy (OMT) or other muscle training and habituation exercises for patients have been a major proactive intervention modality that a dentist or an orthodontist can use. Although the efficacy of OMT is still unclear, it is thought to facilitate remediation for open-bite patients. In this case report, we present the treatment of a patient with an anterior open bite and weak facial muscle force, particularly on the right side, treated with orthodontic appliances combined with OMT. The treatment results were satisfactory, and the patient achieved a good smile and occlusion. An acceptable occlusion and facial proportions were maintained after the 2-year retention period.
Diagnosis and etiology
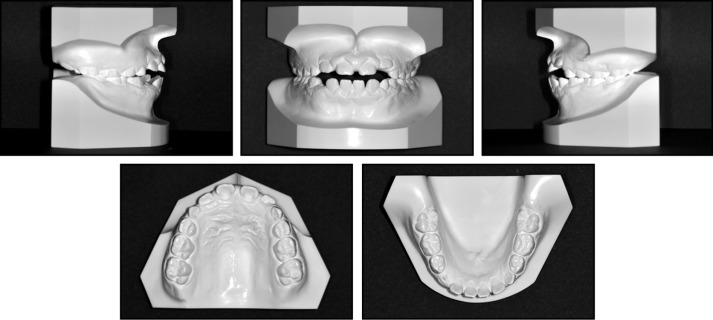
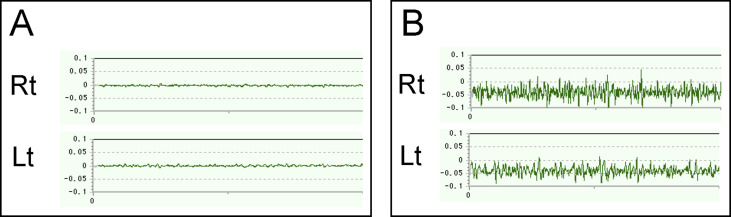
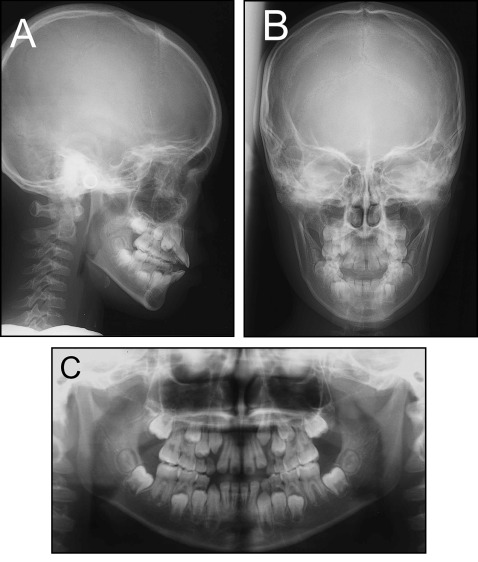
A boy, 10 years 0 months of age, came to the outpatient clinic of Okayama University dental hospital. His chief complaint was an anterior open bite. The facial photographs showed a symmetric face and a straight profile. However, when he smiled, he could not lift his lip on the right side, which was in a flaccid state ( Fig 1 ). Although the origin of his facial soft tissue asymmetry was uncertain, he had a history of open bite since the deciduous dental period, and his saliva often leaked from the right side of his mouth since he was an infant. His symptoms included not being able to enunciate the sounds “ra, ri, ru, re, ro” in Japanese, not being able to blow up a balloon, and not being able to whistle because of the saliva leaking from his mouth. He was not a thumb sucker. Tongue thrust was also observed, but he could not tense his tongue. Additionally, he could not tense his right-side muscles, and his mouth was often open. When he stood straight for a while, his head gradually inclined to the right. He had been taking antiepilepsy drugs since his first seizure at 1 year 2 months of age. Although he experienced provoked seizures several times a year until 5 years of age, further seizures were rare from 5 to 10 years of age. His medical and drug use history showed nothing unusual, except for epilepsy. The intraoral photographs demonstrated gingivitis, possibly associated with taking a steady dose of the antiepilepsy drug. An anterior open bite with a mesial step-type relationship on both sides was observed ( Fig 2 ). A crossbite was not observed in the centric occlusal position, and the midline of the mandibular teeth was deviated to the right by approximately 2 mm to the midline of the maxillary teeth. His occlusion was unstable and showed a left posterior crossbite when he pulled the retractors for his oral photograph, most likely because the right orofacial muscles were too weak to resist the force exerted by the pulling of the left retractor. An electromyographic recording showed weak activity of the masseter ( Fig 3 , A ). A cephalometric analysis, when compared with the normal results for the Japanese population, showed a skeletal Class III relationship (ANB, 1.6°). The maxillary and mandibular incisors were labially inclined (U1-FH, 122.3°; L1-MP, 112.4°), and the interincisal angle was lower (IIA, 97.1°) ( Fig 4 ; Table I ).

| Variables | Mean (10 y) | SD | Mean (adult) | SD | Pretreatment | Before edgewise treatment | Posttreatment | Postretention |
|---|---|---|---|---|---|---|---|---|
| Angular (°) | ||||||||
| ANB | 4.2 | 1.8 | 3.2 | 2.4 | 1.6 | 2.5 | 2.1 | 1.3 |
| SNA | 80.8 | 3.4 | 81.5 | 3.3 | 81.2 | 83.5 | 81.6 | 81.6 |
| SNB | 77.9 | 3.1 | 78.2 | 4.0 | 79.6 | 81.0 | 79.5 | 80.3 |
| Mp-FH | 30.5 | 4.3 | 28.0 | 6.1 | 28.2 | 26.1 | 27.1 | 27.1 |
| Gonial | 122.1 | 5.2 | 120.9 | 6.5 | 121.1 | 123.6 | 124.2 | 124.1 |
| U1-FH | 112.3 | 4.7 | 112.4 | 7.6 | 122.3 | 122.5 | 117.6 | 119.5 |
| L1-Mp | 93.4 | 6.8 | 95.2 | 6.2 | 112.4 | 99.4 | 100.4 | 98.7 |
| IIA | 123.6 | 11.2 | 124.2 | 8.6 | 97.1 | 112.0 | 114.9 | 114.8 |
| Occlusal.plane | 16.9 | 3.7 | 15.5 | 4.2 | 16.4 | 12.4 | 11.6 | 12.1 |
| Linear (mm) | ||||||||
| S-N | 67.9 | 2.5 | 72.2 | 3.3 | 71.6 | 79.0 | 81.6 | 81.6 |
| N-Me | 125.8 | 4.1 | 135.7 | 4.0 | 119.3 | 135.6 | 140.5 | 140.8 |
| Me/NF | 68.6 | 3.3 | 74.6 | 3.0 | 67.1 | 76.3 | 79.7 | 79.9 |
| Ar-Go | 47.3 | 2.6 | 53.2 | 5.7 | 48.9 | 54.9 | 58.4 | 58.4 |
| Ar-Me | 106.6 | 3.0 | 115.6 | 6.8 | 103.6 | 123.2 | 127.3 | 127.4 |
| OJ | 3.1 | 1.4 | 3.3 | 1.0 | 1.8 | 2.6 | 1.9 | 2.0 |
| OB | 3.3 | 2.6 | 3.3 | 1.7 | −4.2 | 0.4 | 1.7 | 1.5 |
| U1-NF | 31.0 | 1.6 | 32.4 | 3.1 | 27.9 | 28.8 | 30.5 | 30.5 |
| L1/MP | 44.2 | 2.1 | 48.9 | 2.6 | 42.4 | 50.6 | 54.0 | 54.1 |
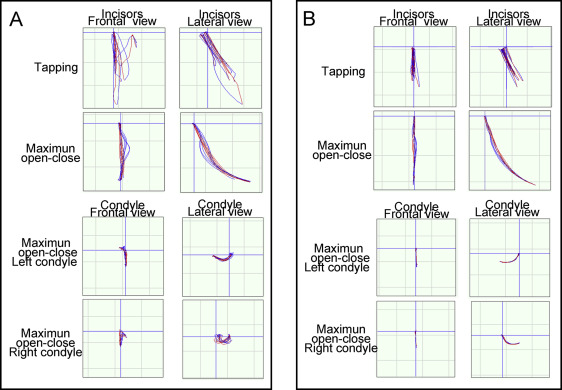
The patient was able to perform the opening and closing and tapping movements, but not the right-left or the anterior gliding movement on a 6 degrees of freedom jaw movement recording system (Gnathohexagraph System version 1.31; Ono Sokki, Kanagawa, Japan). Variability in the condylar movement on the right side during the opening and closing movements was observed. Furthermore, the mandibular incisors often moved to the left during the tapping movement ( Fig 5 , A ).
Based on these findings, the patient was diagnosed with a skeletal Class III jaw base relationship, an anterior open bite, labial inclination of the mandibular and maxillary incisors, and an asymmetrical smile with right perioral muscular weakness.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


