Treatment of a patient with a cleft lip and palate can be challenging. A woman, aged 26 years 8 months, was referred for orthodontic evaluation of her anterior crossbite. She was unhappy with the unesthetic appearance of her maxillary anterior teeth, which were behind her mandibular anterior teeth. She had a unilateral cleft lip and palate and had received primary lip repair and palatoplasty when she was younger, as well as rhinoplasty and a secondary lip repair when she was 15. At the pretreatement evaluation, she had a concave profile with an overjet of −9 mm, a Wits appraisal of −3.8 mm, and a transposed ectopic maxillary right canine. She was treated with orthodontic treatment alone, without orthognathic surgery. The posttreatment records 9 years later showed excellent results with good occlusion, facial balance and harmony, and long-term stability.
Clefts of the lip and palate occur in about 1 in 700 live births in the United States and are the fourth most common craniofacial birth defect. Compared with the incidence rate reported from other countries, the frequency of all forms of clefts is somewhat higher in Asian people than in other races. Not only does the incidence vary between different races, but also the prevalence of cleft type varies by sex. Clefts are caused by failure of fusion between the medial nasal process and the maxillary process, or between the palatal processes. These failures are the combined result of genetic and environmental factors. In cleft patients, dental abnormalities such as hypodontia, malformation, and abnormal eruption pattern occur frequently.
The high prevalence of congenitally missing maxillary lateral incisors is due to a deficiency in the blood supply near the cleft, either congenitally or as a result of surgery, or a deficiency in the mesenchymal support to the maxillary lateral incisor near the cleft. Because a deficiency of the mesenchyme can lead to insufficient mesenchymal support to the bud of the maxillary lateral incisor, cleft patients with a severe deficiency of mesenchymal mass could have congenitally missing maxillary lateral incisors.
Timing and sequencing of orthodontic care for cleft patients can be divided into developmental periods, which are defined by age and dental development and should be considered as time frames in which to accomplish specific objectives.
The purpose of this article is to report the treatment of a woman who had a unilateral cleft lip and palate plus congenitally missing maxillary lateral incisors and a left second premolar. The patient was treated with orthodontics alone; no orthognathic surgery was performed.
Diagnosis and etiology
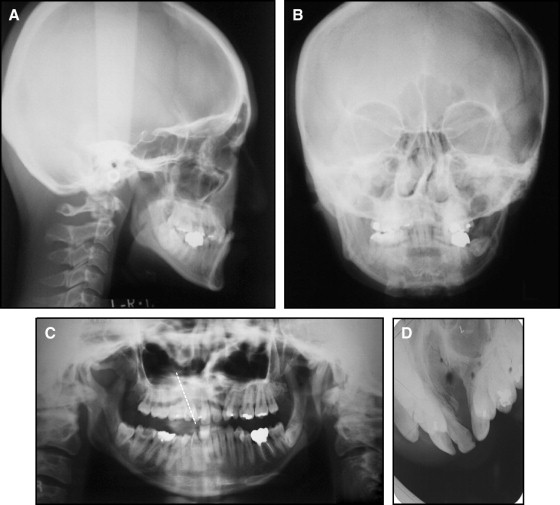
A Japanese woman, aged 26 years 8 months, was referred to an orthodontist for evaluation of her anterior crossbite. Her chief complaint was the unesthetic appearance of her maxillary anterior teeth, which were behind her mandibular anterior teeth. She had a unilateral cleft lip and palate. She had received primary lip repair and palatoplasty, but she could not remember when her operation had been performed. She also had a history of rhinoplasty and a secondary lip repair when she was 15. The patient had a mesofacial and concave profile with a retrusive upper lip and maxilla. Her frontal facial photograph and posteroanterior cephalogram showed a flat alar base and a deviated nasal septum without facial asymmetry ( Figs 1-3 ).

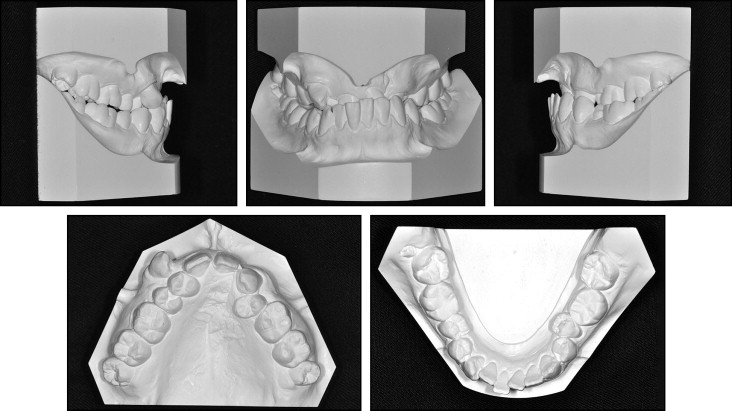
She was congenitally missing her maxillary lateral incisors and a left second premolar. The maxillary arch constriction was due to the unilateral cleft lip and palate. She also had severe crowding in the maxillary arch with anterior and posterior crossbites, and moderate crowding in the mandibular arch with a severe curve of Spee. She had a Class II molar relationship on both sides with an overjet of −9 mm and an overbite of 90%. The maxillary right canine was erupted in an ectopic position. The maxillary left first premolar was rotated 180°. Deep caries was present in the maxillary right second premolar, and secondary caries was developing in the mandibular right first molar and second molar. The maxillary dental midline was deviated to the left by 2 mm relative to the facial midline. It was hard to guide the mandible into centric relation because of the significant arch-size discrepancies.
Cephalometric analysis indicated a skeletal Class III relationship (ANB, −4.7°; Wits appraisal, −3.8 mm) with a normal growth pattern (SN-MP, 35.5°). The maxillary incisors were slightly proclined (U1 to SN, 109.5°), and the mandibular incisors showed retroclination (IMPA, 81.0°) ( Fig 3 , A ; Table ).
| Measurement | Japanese norm | Pretreatment | Posttreatment | 9 years posttreatment |
|---|---|---|---|---|
| SNA (°) | 82.3 | 74.8 | 76.0 | 73.7 |
| SNB (°) | 78.9 | 79.5 | 77.5 | 77.1 |
| ANB (°) | 3.4 | −4.7 | −1.5 | −3.4 |
| Wits (mm) | 0.0 | −3.8 | −1.4 | −2.8 |
| SN-MP (°) | 40.2 | 35.5 | 38.0 | 37.0 |
| FH-MP (°) | 28.8 | 26.6 | 29.0 | 27.8 |
| LFH (ANS-Me/N-Me) (%) | 55.0 | 55.0 | 58.0 | 57.0 |
| U1 to SN (°) | 104.5 | 109.5 | 121.0 | 121.0 |
| U1 to NA (°) | 22.0 | 35.0 | 47.1 | 47.6 |
| IMPA (°) | 96.3 | 81.0 | 82.5 | 80.0 |
| L1 to NB (°) | 25.0 | 15.0 | 14.9 | 12.2 |
| U1/L1 (°) | 124.1 | 134.0 | 121.1 | 123.5 |
| Upper lip (mm) | 1.2 | −5.8 | −2.4 | −4.1 |
| Lower lip (mm) | 2.0 | −0.8 | −2.0 | −2.0 |
The panoramic radiograph showed that the crown of the mandibular left third molar was overlapping the distal root of the mandibular left second molar. The ectopic canine had a transposed root with the maxillary right first premolar ( Fig 3 , C ).
Treatment objectives and alternatives
The treatment objectives were to obtain normal overjet and overbite, establish a Class I canine relationship, maintain a Class II molar relationship, correct the midline shift, relieve the crowding in both arches, and level the curve of Spee. In addition to better occlusion, improvement of the patient’s profile was also crucial. Careful observation of the maxilla was required during treatment because she had had surgical lip repair and palatal closure.
To accomplish these objectives, forward movement of the premaxilla was planned, followed by lateral expansion of the buccal dentition. It was expected that her facial profile would improve after these treatments. Lip and nose revisions were also considered. It was presumed that the labial and lateral expansions would enlarge the maxillary left alveolar cleft, so a secondary bone graft was considered to close these clefts at an appropriate stage, but the patient declined the procedure. A conventional fixed prosthesis or a dental implant was planned for the missing tooth after the orthodontic treatment.
As a treatment alternative, orthognathic surgery without intensive maxillary arch expansion was considered. This plan would correct the crossbite and improve the facial profile. Using conventional orthognathic surgery techniques for patients with severe maxillary hypoplasia, surgeons would advance the maxilla as much as possible in the presence of the scar tissues from the lip and palate repairs. The remaining skeletal discrepancy would be corrected with a mandibular setback. Essentially, this would be a surgical camouflage of the inability to correct the underlying maxillary hypoplasia predictably. Additionally, the velopharyngeal mechanism could be compromised by maxillary advancement, especially if a pharyngeal flap was used to improve speech.
Details of these alternatives were presented to the patient; however, she declined the surgery. Because of this, we decided on orthodontic treatment alone. We expected that expansion of the maxillary arch at her age would help to correct the posterior crossbite mostly by buccal tipping. Opening the space for the maxillary left lateral incisor would be helpful to expand the premaxilla. We planned to consider orthognathic surgery later, if the results of orthodontic treatment were not acceptable.
Treatment objectives and alternatives
The treatment objectives were to obtain normal overjet and overbite, establish a Class I canine relationship, maintain a Class II molar relationship, correct the midline shift, relieve the crowding in both arches, and level the curve of Spee. In addition to better occlusion, improvement of the patient’s profile was also crucial. Careful observation of the maxilla was required during treatment because she had had surgical lip repair and palatal closure.
To accomplish these objectives, forward movement of the premaxilla was planned, followed by lateral expansion of the buccal dentition. It was expected that her facial profile would improve after these treatments. Lip and nose revisions were also considered. It was presumed that the labial and lateral expansions would enlarge the maxillary left alveolar cleft, so a secondary bone graft was considered to close these clefts at an appropriate stage, but the patient declined the procedure. A conventional fixed prosthesis or a dental implant was planned for the missing tooth after the orthodontic treatment.
As a treatment alternative, orthognathic surgery without intensive maxillary arch expansion was considered. This plan would correct the crossbite and improve the facial profile. Using conventional orthognathic surgery techniques for patients with severe maxillary hypoplasia, surgeons would advance the maxilla as much as possible in the presence of the scar tissues from the lip and palate repairs. The remaining skeletal discrepancy would be corrected with a mandibular setback. Essentially, this would be a surgical camouflage of the inability to correct the underlying maxillary hypoplasia predictably. Additionally, the velopharyngeal mechanism could be compromised by maxillary advancement, especially if a pharyngeal flap was used to improve speech.
Details of these alternatives were presented to the patient; however, she declined the surgery. Because of this, we decided on orthodontic treatment alone. We expected that expansion of the maxillary arch at her age would help to correct the posterior crossbite mostly by buccal tipping. Opening the space for the maxillary left lateral incisor would be helpful to expand the premaxilla. We planned to consider orthognathic surgery later, if the results of orthodontic treatment were not acceptable.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


