An 8-year-old girl with a skeletal Class III malocclusion was treated in 2 phases. Maxillary expansion and protraction were carried out as the early intervention. However, her maxillary hypoplasia and mandibular hyperplasia deteriorated with age. The phase 2 comprehensive treatment began with proper mechanics when she was 12 years old with growth potential. In the maxillary arch, an auxiliary rectangular wire was used with a round main wire and an opening spring to create space for the impacted teeth and to bodily move the anterior teeth forward. Decompensation of mandibular incisors and correction of the Class III malocclusion were achieved by short Class III elastics with light forces and a gentle interaction between the rectangular wires and the lingual root-torque slots. The phase 2 active treatment period was 4 years 8 months. The 2-year follow-up indicated that our treatment results were quite stable.
In the treatment of skeletal Class III malocclusion, there is no clear borderline between what can be achieved by orthodontic camouflage and what inevitably requires orthognathic surgery. Comparatively, orthognathic surgery could obtain substantial skeletal improvement as well as favorable tooth inclinations by the presurgical decompensation. However, camouflage treatment demands more time and high patient compliance, although the treatment expenses and risks are lower. For patients who do not want the risk of surgery, early orthodontic intervention in the mixed dentition followed by comprehensive treatment in the early permanent dentition is a valid therapy.
Traditional orthodontic camouflage of skeletal Class III malocclusion always results in more lingual inclination of the mandibular incisors and more proclination of the maxillary incisors for compensation of a skeletal discrepancy. However, excessive inclination of the incisors will not only ruin the dental esthetics but also harm the surrounding periodontal tissues, probably from the traumatic occlusal forces. Authors of a previous study attempted to improve the compensative inclination of the mandibular incisors with mandibular skeletal anchorage.
The patient’s pubertal growth is the optimal timing for routine orthodontic treatment because modifications of dentoalveolar bone are easier in this stage. In general, bone around the alveolar socket will remodel to the some extent after orthodontic tooth movement. If orthodontists could take the advantage of this period to achieve “orthodontic decompensation” and to correct a Class III malocclusion at the same time by gradual alveolar remodeling with comprehensive orthodontic treatment, further inclination of the incisors and unfavorable side effects could be avoided. How much could the dentoalveolar remodeling compensate for the base bone discrepancy? To answer this question, we present a skeletal Class III patient treated with early intervention and orthodontic camouflage. In her comprehensive orthodontic treatment, we attempted to decompensate the incisor inclination during her growing stage with dentoaveolar remodeling.
Diagnosis and etiology
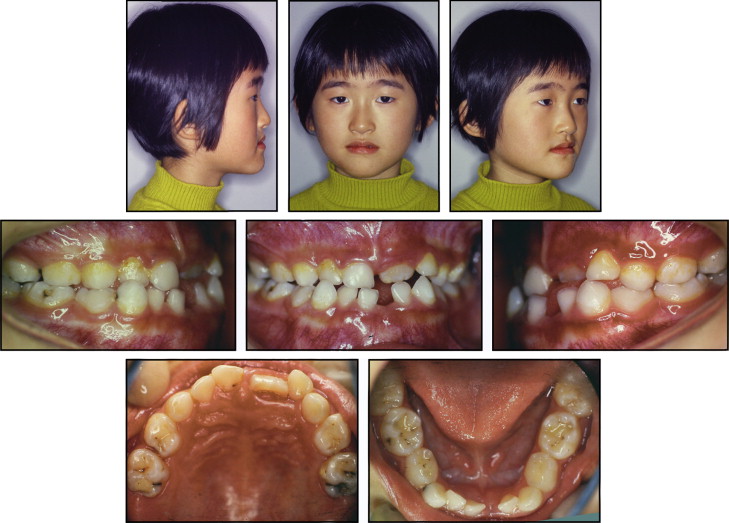
An 8-year-old girl came for orthodontic consultation with chief complaints of an anterior crossbite and a dished-in face. Her parents said that her psychology was negatively affected by her unesthetic facial appearance. Her medical history showed no systemic diseases or developmental anomalies. Her parents did not have Class III characteristics.
The patient had a retrognathic maxilla and a prognathic mandible with a sharp nasolabial angle and a concave facial profile ( Fig 1 ). As shown by the cephalometric analysis, the ANB angle was −3.5°, and the Wits appraisal was −6.5 mm ( Fig 2 , Table ). The intraoral examination indicated a Class III malocclusion with an anterior crossbite and a unilateral crossbite. Cephalometrically, she had lingually inclined mandibular deciduous incisors (Md 1 to MP, 66.8°) and an excessive interincisal angle (166.1°), which was the dental compensation of the skeletal Class III discrepancy. Her cephalogram showed that the lower border of the second through the fourth cervical vertebrae had no concavity, indicating that she was at cervical vertebral stage 1.