History of the Procedure
A court physician to the king of Württemberg, Wilhelm Friedrich von Ludwig, described the well-known condition of Ludwig’s angina in 1836, but not until the early twentieth century was the relationship between dental abscess and severe life-threatening neck swelling established. Incision and drainage of odontogenic abscess, in addition to dental extraction, has been a time-honored procedure performed by oral and maxillofacial surgeons. This operation relies on a thorough understanding of the fascial layers and the potential anatomic spaces through which infection can spread in the head and neck, as published in the classic anatomic studies done by Grodinsky and Holyoke in 1938-1939. Prior to that, head and neck infection was common and often lethal. Osteomyelitis of the jaws was also a common and serious problem. At that time, erysipelas carried a 60% mortality rate. A discussion of the history of odontogenic infections is not complete without acknowledging the work in the modern and classic Oral and Maxillofacial Infections textbook by Topazian and Goldberg.
History of the Procedure
A court physician to the king of Württemberg, Wilhelm Friedrich von Ludwig, described the well-known condition of Ludwig’s angina in 1836, but not until the early twentieth century was the relationship between dental abscess and severe life-threatening neck swelling established. Incision and drainage of odontogenic abscess, in addition to dental extraction, has been a time-honored procedure performed by oral and maxillofacial surgeons. This operation relies on a thorough understanding of the fascial layers and the potential anatomic spaces through which infection can spread in the head and neck, as published in the classic anatomic studies done by Grodinsky and Holyoke in 1938-1939. Prior to that, head and neck infection was common and often lethal. Osteomyelitis of the jaws was also a common and serious problem. At that time, erysipelas carried a 60% mortality rate. A discussion of the history of odontogenic infections is not complete without acknowledging the work in the modern and classic Oral and Maxillofacial Infections textbook by Topazian and Goldberg.
Indications for the Use of the Procedure
Odontogenic infection with clinical or radiologic evidence of abscess collection warrants incision and drainage via either a transcutaneous or a transoral approach, depending on the space involved, in addition to dental extraction. Modern protocols typically supplement the physical examination with a computed tomography (CT) scan with intravenous contrast dye to delineate the presence of collection and to localize the fascial spaces involved. Fascial space infection associated with an odontogenic source may include one or a combination of the spaces represented in Box 17-1 .
Deep fascial space infection associated with any tooth:
- •
Vestibular
- •
Buccal
- •
Subcutaneous
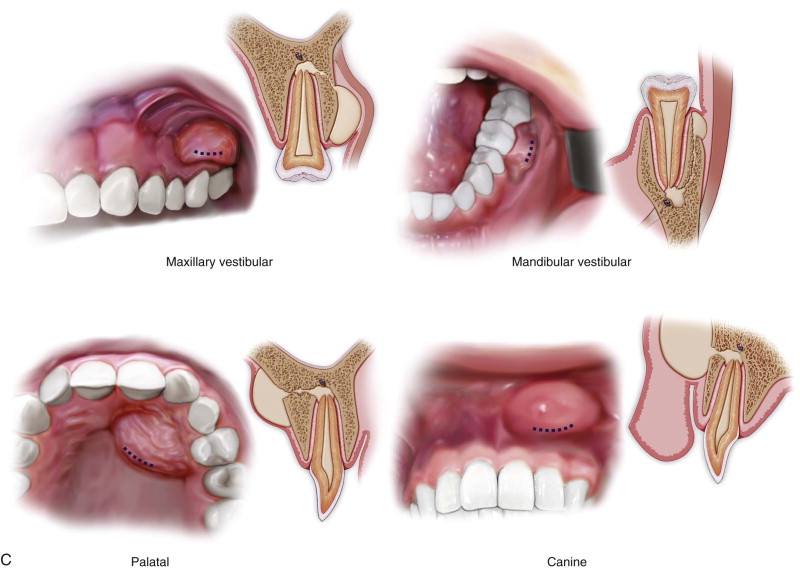
Deep fascial space infections associated with maxillary teeth:
- •
Canine
- •
Palatal
- •
Buccal
- •
Infratemporal
- •
Maxillary and other paranasal sinuses
- •
Cavernous sinus thrombosis
Deep fascial space infection associated with mandibular teeth:
- •
Space of the body of the mandible
- •
Submandibular
- •
Sublingual
- •
Submental
- •
Masticator (submasseteric, pterygomandibular, superficial temporal, deep temporal)
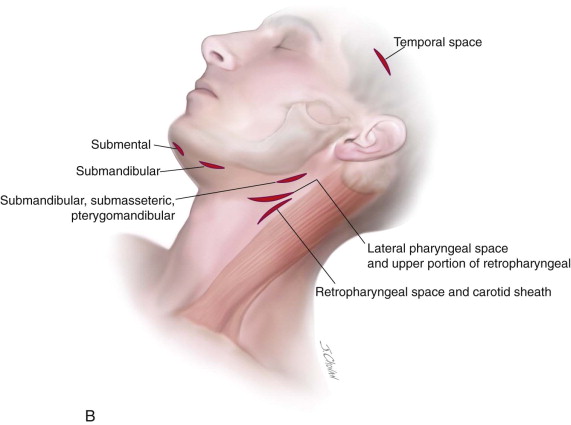
Deep fascial space infection of the neck and chest:
- •
Lateral pharyngeal (anterior and posterior compartments)
- •
Retropharyngeal
- •
Pretracheal
- •
Prevertebral
- •
Danger space
- •
Prevertebral
- •
Mediastinum
Limitations and Contraindications
The practice of incision and drainage, along with eradication of the source of infection, is considered an urgent procedure and is rarely contraindicated in most circumstances. Trismus can make extractions and transoral approaches to drain the abscess challenging under local anesthesia, and many times general anesthesia is required. Medical comorbidities may require perioperative modification to optimize the patient for surgery and also may contribute to a poor or prolonged postoperative resolution of the infection.
Technique: Incision and Drainage of Fascial Space Infection of Odontogenic Origin
Step 1:
Securing Airway
Establishing a secure airway is paramount in cases of severe deep neck infection. Awake or sedated fiberoptic intubation might be necessary in cases of severe trismus or other airway compromise. Nasal intubation is relatively contraindicated in cases of retropharyngeal abscess due to potential iatrogenic disruption of posterior pharyngeal wall mucosa, increasing the risk of aspiration of infected material. The surgeon should be prepared to perform surgical airway placement if a “cannot intubate, cannot ventilate” situation is encountered.
Step 2:
Aspiration of Abscess
After application of topical cutaneous cleansing agent, abscess material is aspirated transcutaneously with a 10-cc syringe connected to an 18-g needle in a sterile fashion. If transmucosal aspiration is planned, a chlorhexidine oral rinse should be applied to minimize oral flora contamination. Aspirate should be sent as a microbiologic culture specimen ( Figure 17-1, A ).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


