A 15.3-year-old white girl with a skeletal Class III malocclusion and a severe lateral open bite was treated with conventional orthodontics and directional force mechanics and elastics. She had 5 congenitally missing premolars. The maxillary right canine was ectopically erupted and in contact with the maxillary right first molar. An Angle Class I molar relationship was achieved with canine protected occlusion and incisal guidance. A wrap-around retainer was placed on the maxillary arch and a lingual bonded retainer on the mandibular arch. Treatment time was 38 months.
Edward H. Angle described a Class III malocclusion as a condition in which the mandibular first molar is positioned mesially to the maxillary first molar. This relationship could include a skeletally recessive maxilla and a normal mandible, a prognathic mandible and a normal maxilla, or a combination of both. This dental relationship could also have a normal maxillary-mandibular relationship. The treatment of choice is normally to correct the faulty skeletal component and the dental malrelationship. A pseudo-Class III can be caused by a forward shift of the mandible to avoid incisal interferences. In the United States, true Class III malocclusions are found in less than 1% of the general population.
An open bite with any malocclusion classification is a difficult and complex anomaly to correct. It is particularly troublesome when it is associated with a Class III malocclusion. Open bite can be caused by an abnormal growth pattern, finger sucking, airway obstruction, or tongue posture and function.
Class III malocclusions are difficult for treatment planning. The clinician must choose either a camouflage treatment to mask the Class III malocclusion or a surgical alternative to correct the skeletal imbalance. Certainly, an open bite, whether it is lateral or anterior, complicates the Class III correction. In many instances, it can make the Class III malocclusion worse. What if the patient grows? What if the patient’s parents are adamantly opposed to surgery? Can a nonsurgical compromise be accomplished, even if it is not the optimum choice? All these questions must be answered by the clinician in planning treatment to correct the patient’s malocclusion.
Diagnosis and etiology
The patient was a white girl, aged 15.3 years, with an unremarkable medical history. She had a Class III dental malocclusion, a lateral open bite, and a slightly convex facial profile. Her maxilla appeared to be recessive. The maxillary right canine erupted next to the maxillary right first permanent molar. Her chief concerns were “my underbite and my side teeth don’t touch.” The primary etiology was heredity.
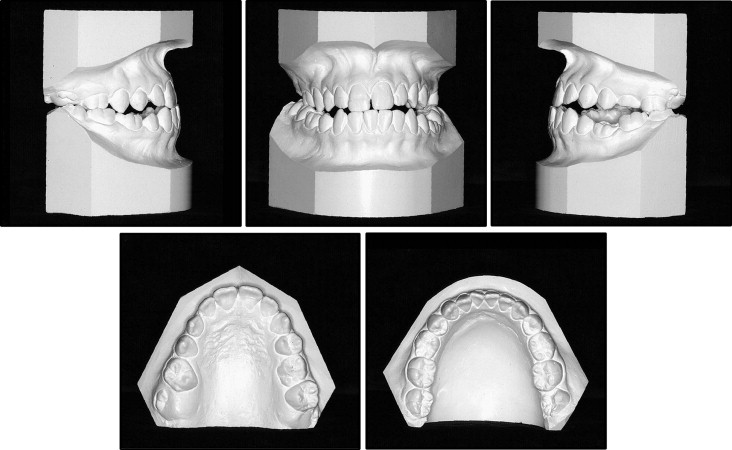
The facial and intraoral photographs ( Fig 1 ) demonstrate a slightly convex facial profile. The patient was able to close her lips without mentalis strain. The maxillary midline was deviated toward her left.

The dental casts ( Fig 2 ) show an Angle Class III occlusion on the left and a Class I dental relationship on the right. The maxillary right canine had erupted ectopically next to the maxillary right first molar and was in an extreme Class III position in relation to the mandibular right canine. The maxillary right deciduous canine was present in the permanent canine position. The maxillary left second deciduous molar was present. The mandibular second deciduous molars were also present. There was a crossbite of the maxillary teeth on the right and a negative overjet of −1 mm. There was 1 mm of mandibular anterior crowding. Lateral open bites of 6 mm on the right and 5 mm on the left were present. The maxillary second molars were not erupted. Her teeth occluded only on the terminal molars. The midlines deviated by 3 mm.
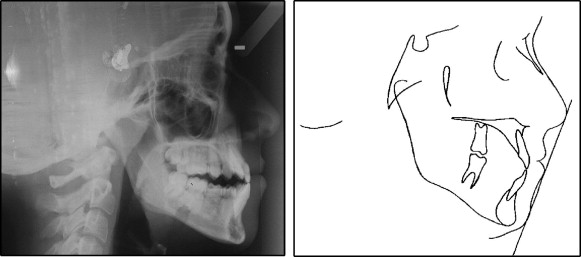
The pretreatment cephalogram and its tracing ( Fig 3 ) showed an ANB angle of 1°. The Wits appraisal of −8 mm confirmed a skeletal Class III alveolar imbalance. The FMA of 30° suggested a vertical skeletal discrepancy. The facial height index (posterior facial height/anterior facial height) of .78 suggested a skeletal deepbite tendency. The Z-angle of 69° confirmed a mildly protruded soft-tissue overlay. The incisors were not in contact. The panoramic radiograph ( Fig 4 ) showed that the maxillary right first and second premolars, the maxillary left second premolar, the mandibular second premolars, and all third molars were congenitally missing. The maxillary left second deciduous molar, the maxillary right deciduous canine, and the mandibular second deciduous molars were present. The maxillary second permanent molars were unerupted.

After the casts, the radiographs, the photos, and the patient were studied, it was decided to approach her problem as a Class III open-bite correction.
Treatment objectives
The treatement objectives were to (1) obtain a normal profile line to nose relationship and a normal Z-angle, (2) obtain normal canine and incisal guidance, (3) correct the lateral open bite, (4) correct the Class III dental relationship, (5) place the maxillary right canine in its correct Class I position, (6) place the dental midlines in the middle of the patient’s face, and (7) prepare the dentition to be prosthetically restored.
Treatment objectives
The treatement objectives were to (1) obtain a normal profile line to nose relationship and a normal Z-angle, (2) obtain normal canine and incisal guidance, (3) correct the lateral open bite, (4) correct the Class III dental relationship, (5) place the maxillary right canine in its correct Class I position, (6) place the dental midlines in the middle of the patient’s face, and (7) prepare the dentition to be prosthetically restored.
Treatment alternatives
- 1.
Extract the mandibular left and right deciduous molars and upright the mandibular incisors over basal bone. Extract the maxillary right deciduous canine and move the right permanent canine forward to contact the maxillary right lateral incisor to create space for premolar replacement. The maxillary left second deciduous molar would be left in place to maintain space for an osseointegrated implant crown, and the maxillary left first molar would occlude with the mandibular left second molar in a Class I relationship. The maxillary left second molar would be without an antagonist tooth.
- 2.
Level both arches and maintain all remaining deciduous teeth in their current positions for prosthetic replacements except for the maxillary right deciduous canine. The maxillary right deciduous canine would be extracted to allow the maxillary right permanent canine to be moved mesially to contact the right lateral incisor so that space could be gained for a premolar implant. After leveling and detailing the arches with this plan, a maxillary LeFort impaction and a mandibular setback osteotomy would correct the open bite, the crossbite, and the Class III dental relationship. The patient’s parents were adamantly opposed to surgery and the added expense of implants to replace the congenitally missing teeth.
Treatment plan
Merrifield’s total space analysis was used to determine space requirements. A decision was made to extract the mandibular second deciduous molars. The extraction of these teeth would provide space to further upright the mandibular incisors over basal bone. This uprighting movement would help correct the Class III appearance and improve the Z-angle. The maxillary right deciduous canine would be extracted so that the maxillary canine could be positioned in its proper place in the arch. The maxillary left second deciduous molar would be retained to prevent mesial movement of the maxillary left first molar. The maxillary left second molar would have no antagonist with this plan.
Treatment progress
All teeth were sequentially banded or bonded with a 0.022-in standard nontorqued, nonangulated edgewise appliance. The 10-2 system of Merrifield was used. A hyrax expander was placed and given 2 turns per day to open the midpalatal suture or to at least gain some expansion to correct the posterior crossbite. Triangular and vertical elastics were used to help control the bite opening that this widening of the palate would create. After 15 days with the expander, the posterior crossbite was corrected, and the appliance was stabilized.
At the same time, the patient was instructed to wear a J-hook straight-pull headgear with the J-hooks placed directly against the mandibular canine brackets to move the mandibular canines and first premolars distally. Mandibular canine and premolar retraction was augmented with elastic power chains. When the canines and first premolars were completely retracted, the mandibular incisors were retracted with a 0.021 × 0.025-in closing-loop archwire. A high-pull J-hook headgear was attached to hooks soldered on the archwire between the mandibular central and lateral incisors. The maxillary expander was left in place for almost 24 months so that it could serve as an anchor unit, while the maxillary right canine was moved mesially with an open coil on the archwire.
Toward the end of treatment, when the maxillary right canine was in its proper position, and the hyrax appliance was removed, the maxillary right first molar remained in a Class III relationship. The space remaining was too large for 1 implant and too small for 2. One implant was placed. After it had integrated, a temporary crown was placed so that the implant could be used to close the excess space and serve as an anchor to bring the maxillary right first molar into a Class I dental relationship.
The patient’s mother had unreasonable expectations and objectives during most of the treatment. She absolutely could not accept orthognathic surgery and had to be convinced that an implant was necessary. She agreed only to the implant in the maxillary right quadrant because the tooth was missing. Fortunately, the patient was wonderfully compliant and did not grow. The family was informed that the maxillary left second deciduous molar will need to be replaced eventually by an implant and a crown.
Vertical, triangular, and Class III elastics were used as needed. When a Class I canine relationship was achieved on the right side and the open bite had been corrected, the maxillary right first molar remained in a Class III position. At this time, an implant was inserted to replace the missing maxillary right premolar. Ideal finishing wires stabilized the teeth, while the implant osseointegrated and the occlusion settled. After the implant was integrated, a temporary crown was placed. The implant crown was banded and used to move the right first molar mesially into a Class I position. The maxillary left first molar occluded with the mandibular left second molar in an end-on Class I dental relationship. The maxillary left second molar has no antagonist. A maxillary wrap-around retainer and a mandibular bonded retainer were placed. Total treatment time was 38 months.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


