Non-surgical Re-treatment Case III:
Mandibular Molar
Bruce Y. Cha

Chief Complaint
“Swelling on the gum near the last molar on the right side of the lower jaw. It is painful to touch. My face is swollen, too.”
Medical History
The patient (Pt) was a 72-year-old Caucasian female. She took Synthroid® 0.025 mg daily for hypothyroidism, Meloxicam 7.5 mg daily for arthritis, and Lexapro® 10 mg once daily for depression. She also used an estrogen patch daily and Restasis® drops for dry eyes. She had been taking ProlixTM injections for postmenopausal osteoporosis for ten years.
She had adverse gastrointestinal reactions to penicillin, clindamycin, and Flagyl®. She was a non-smoker and a retired educator.
The Pt was considered American Society of Anesthesiologists Physical Status Scale (ASA) Class II.
Dental History
The Pt started to experience severe pain on tooth #31 and swelling in the adjacent gum tissue during the previous weekend. She also noticed that her face became swollen. Her general dentist put her on Keflex® 500 mg three times daily which made her pain and swelling more tolerable. When tooth #31 had root canal treatment (RCT) about ten years ago, the Pt was told that the tooth had a hairline crack at the distal marginal ridge. The Pt did not remember any specific information related to RCT done for tooth #30. She indicated her anxiety about dental procedures in general and was concerned about potential osteonecrosis of the jaw related to her current medication if the tooth should be extracted.
Clinical Evaluation: Diagnostic Procedures
Examinations
Extra-oral Examination (EOE)
The Pt seemed to be in acute distress. The Pt’s face was swollen on the right side. Clinical examination revealed lymphadenopathy on the right submandibular area. The body temperature was 98.4° F. The Pt had trismus related to facial swelling. However, the tempromandibular joint was within normal limits (WNL) without symptoms and signs of popping and clicking.
Intra-oral Examination (IOE)
The gum was swollen at the buccal (B) area of tooth #31 and was sensitive to palpation. Tooth #31 was remarkably sensitive to percussion with class 2 mobility. The margin of crown on tooth #31 was intact. Periodontal probing was not performed due to the pain and swelling in the gum.
Diagnostic Tests
| Tooth | #31 | #30 |
| Percussion | ++ | – |
| Palpation | ++ | – |
| Cold | N/A | N/A |
| Mobility | Yes | No |
| EPT | N/A | N/A |
| Swelling | ++ | + |
EPT: Electric pulp test; ++: Percussion/ palpation/swelling significant; +: Swelling exists; –: No response to percussion/palpation; N/A: Not applicable
Radiographic Findings
In the 2-D periapical radiograph (Figure 18.1), there seemed to be periapical radiolucency (PARL) with loss of lamina dura present at the apex of the mesial (M) root of tooth #31. The PARL at the M root extended to the M area of the distal (D) root apex. There was a full crown with amalgam restoration at the M area. A threaded post in the D root showed a 2 mm gap apically to the root canal filling. The root canal fillings in both roots reached 1 mm point from the radiographic apices. Sclerosis of the bone was observed in the periapical bone or the D root of tooth #31 and in the periapical bone of both roots of tooth #30. The D root canal filling of tooth #30 was underextended by 3 mm. Slight crestal bone loss was noticed at the interproximal bone between teeth #31 and #30. Widened periodontal ligament (PDL) and mild vertical bone loss was present at the distal of tooth #31. The furcation was intact on both teeth #31 and #30.
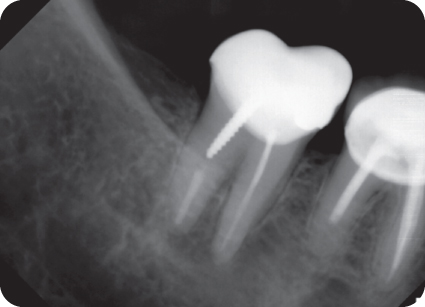
Figure 18.1 Preoperative 2-D radiograph showing hint of periapical radiolucency mesial root of tooth #31.
In the limited-view 3-D cone beam-computed tomography (CBCT) image (Figure 18.2) taken with Kodak 9000 3-D System field of view 50 x 37 mm at voxel size 76 µm (Carestream, Rochester, NY, USA), all axial, sagittal, and coronal slices of each scan were evaluated with the software provided with the CBCT unit. Scans were viewed in a clinical environment on 24-inch monitors (resolution 1920 x 1200 at 60 Hz). Axial, sagittal, and coronal images of each root were examined by aligning the slicing line parallel to the long axes of each canal. In axial view, a definite radiolucency with diffuse border and a diameter of 9 mm circumscribing the M root apex was noticed. The coronal part of the root canal filling in the M root was located slightly off-center towards the B aspect. In sagittal view, the distal border of the radiolucency extended to the D root of tooth #31 and to the inferior border of the lesion encroached to the inferior alveolar nerve canal. The coronal view confirmed the proximity of the lesion to the inferior alveolar nerve which was located 8 mm apical from the apex of the M root. The coronal portion of the root canal filling in the M root was located off-center towards the B aspect as in axial view. In the coronal part, radiolucent canal space suggestive of previously untreated mesiolingual (ML) canal was visible lingual (L) to the root canal filling. In the apical part, the gutta-percha (GP) filling was located in the center of the root in buccolingual (BL) dimension, which suggested merging of MB and ML canals to form one apical foramen. The periapical tissue of both roots of tooth #30 were WNL with normal trabeculation.

Figure 18.2 Comparison of preoperative 2-D radiograph and 3-D CBCT image showing the enhanced clarity of the periapical in 3-D CBCT imaging.
Pretreatment Diagnosis
Pulpal
Previously Treated with the exception of ML canal, tooth #31
Apical
Acute Apical Abscess, tooth #31
Treatment Plan
Recommended
Emergency:To obtain drainageDefinitive:Non-surgical (Selective) Root Canal Re-treatment of tooth #31
Alternative
Extraction and dental implant or surgical endodontics
Restorative
Restoration of the endodontic access with amalgam.
Replacement of the crown if there is recurrent caries under the crown which compromises the marginal seal.
Prognosis
| Favorable | Questionable | Unfavorable |
| X |
Clinical Procedures: Treatment Record
First visit (Day 1): Anesthesia: 54 mg of 3% mepivacaine was administered for inferior alveolar nerve block (IANB) and 36 mg of 2% lidocaine (lido) with 1:100,000 epinephrine (epi) (0.018 mg) was administered for long buccal nerve block. Dental dam isolation was achieved using Ivory® 12A clamp (Heraeus Kulzer, Hanau, Germany). Indirect visualization was obtained with a dental mirror through the dental operating microscope (DOM; Zeiss OPMI®, Oberkochen, Germany). Endodontic access was made through the metal occlusal surface of the crown. Initial penetration was made with a #2 round bur mounted on high speed handpiece. A Great WhiteTM fissure bur (SS White®, Lakewood, NJ, USA) was used to enlarge the endodontic access, and the M wall of the access was slightly flared occlusally to aid the visualization and the approach of the instruments to the canals. The outline of the endodontic access was shaped as a triangle with a rounded vertex located near the central fossa and the edge of the triangle facing the M marginal ridge of the crown. A surgical length #4 round bur was used in the deeper level excavation of the previous core buildup materials. The visualization of the post and core build up at the D part of the chamber showed no contamination from microleakage. The amalgam restoration at the M area was carefully excavated without water coolant, with air spray to blow off dust which was evacuated with suction for optimal visualization. Slight leakage was seen along the margin of the amalgam restoration. The positions of the chair and the head rest were frequently adjusted to maintain maximum visualization. The B swelling and trismus impaired visualization of the access process, especially for the ML that required the retraction of the DB curtain of soft tissues. A surgical length #2 round bur was used as the excavation process approached the deeper level of the chamber floor in order to minimize unnecessary removal of supportive dentin. The use of the DOM, which provided magnification with illumination powered by Xenon light source, allowed the clinician to discern the subtle difference between the restorative materials and the dentin.
Careful excavation continued with surgical length #2 round bur on the floor of the chamber in search for the orifi of the M canals. In this process, shaving of the dentin layer was followed by air spray for visual inspection. The procedure was executed repeatedly in many small steps in order to avoid accidental perforation of the floor of the chamber and also to preserve dentin. Once the GP in the MB canal was spotted, the search was directed towards the L area to locate the orifice of the ML canal. An endodontic explorer was used to probe the chamber floor in searching for the ML orifice which was discovered slightly L of the GP filling in the MB canal (Figure 18.3). The visual examination revealed dark matter contained in the ML canal. This finding was suggestive of contamination with polymicrobial infection and microleakage. There was a typical anaerobic odor upon discovery of the orifice. The 3-D CBCT image was frequently used as a visual reference in searching for the ML orifice using DOM (Figure 18.4).

Figure 18.3 Clinical photograph taken with dental operating microscope. View showing contaminated ML canal which was previously untreated. The gutta-percha in MB canal is contiguous with ML canal space. The distal part of the composite core build up with post was intact without leakage. Slight recurrent caries shown at the amalgam restoration at the mesial area.

Figure 18.4 The juxtaposition of 3-D CBCT diagnostic imaging and the view through the dental operating microscope (×5.1) correlates the diagnostic imaging with operating field inside the pulp chamber.
The contaminated root canal space of ML was initially accessed with a size #15 K-file in the coronal portion. The tactile sensation indicated that the ML and the GP in the B aspect were contiguous without isthmus in the mid-root level. Using size #20 and size #25 Hedstrom files, the contamination in the coronal portion of the ML canal was cleaned. Then, size #2 and #3 Gates-Glidden burs were used in both MB and ML canals to secure the coronal access. Chloroform was sparingly applied to facilitate the removal of the GP in the MB canal. A crown-down approach was taken to minimize the iatrogenic irritation to the inflamed periapical tissue. Continued use of Hedstrom files enabled the removal of the GP in MB canal (Figure 18.5). Approaching the apical portion of the canal, working length (WL) was measured with a radiograph taken with a size #25 K-file (Figure 18.6). The determined WL was 18 mm measured on the MB line angle of the endodontic access. Apical patency was checked with a size #10 K-file. There was no drainage coming through the canal.

Figure 18.5 Clinical photograph taken with dental operating microscope view after instrumentation and disinfection of ML and MB canals. The gutta-percha in MB canal had been removed.

Figure 18.6 Working radiograph measuring the length of the canal.
During the biomechanical instrumentation process, the residues of GP and sealer from the previous treatment were removed with sequential use of K-files and Hedstrom files. Rotary files were also used for the shaping process. 2.5% sodium hypochlorite (NaOCl) and 17% ethylenediaminetetraacetic acid (EDTA) were used as irrigating solutions. An ultrasonic tip (SybronEndo) was used to clean the dentinal walls. The cleanliness and shaped canals were visualized with the DOM after the drying process with size #30, .04 taper paper points. The placement of paper points confirmed the shape of two canals merged to one apical foramen. Calcium hydroxide (Ca(OH)2) was placed in the canals with injection using a 23 gauge needle. A size #30 file was used to spread Ca(OH)2 to the WL. Polytetrafluoroethylene (PTFE) tape was placed over the Ca(OH)2, and Cavit™ (3M, Two Harbors, MN, USA) was used for temporization. After the dental dam was removed, occlusion was checked, including the contact during the lateral excursion.
Performing an incision and drainage (I&D) procedure was discussed with the Pt as drainage was not achieved through the root canal space. The Pt declined to have the I&D at this appointment and was willing to wait and see how the swelling and lymphadenopathy responded in the following 2–3 days. Postoperative (PO) care information was given. The Pt was instructed to continue with the current antibiotic regimen of Keflex. Ibuprofen 600 mg was prescribed on an as needed basis for PO discomfort.
Second visit (Day 16): Pt presented with comfortable condition in tooth #31. With swelling fully reduced, she complained of mild tightness of the muscle on the B area from the previous swelling. There was no pocket probing more than 3 mm. Anesthesia was administered with 54 mg of 3% mepivacaine for IANB and 18 mg of 2% lido with 1:100,000 epi (0.009mg) for long buccal nerve block. Tooth #31 was isolated with a dental dam using Ivory® 12A clamp (Heraeus Kulzer, Wehrheim, Germany). Endodontic access was re-established by removing the Cavit™ and PTFE placed in the pulp chamber. Ca(OH)2 was removed with irrigation of 2.5% NaOCl. The mesial canals were cleaned and shaped with the sequential use of K-, Hedstrom, and rotary files according to the established WL. Then, the canals were dried with size #30, .04 taper sterilized paper points. A size #30 master GP cone was fitted to the WL, and its apical termination was verified with a radiograph. First, the canals were filled with AH26® Root Canal Sealer (Dentsply Sirona, Konstanz, Germany). Then, the master cone was placed, followed by the alternating steps of spreading the space with D-11 and inserting .04 taper fine accessory points. The GP mass was heated with System B™ (Kerr, Orange, CA, USA) in order to facilitate the lateral condensation process. The root canal obturation process was monitored with a radiograph (Figure 18.7). Excess endodontic sealer was removed by cleaning the chamber with 70% alcohol followed by a washing and drying process. After having discussed how to restore the endodontic access with the referring general dentist on the phone, amalgam was condensed in the endodontic access of the crown. After the dental dam was removed, occlusion was checked, a final radiograph was taken (Figure 18.8), and PO instruction was provided. The Pt was instructed to take over-the-counter ibuprofen 200 mg to 400 mg every 4–6 hours as needed for PO discomfort. The Pt made arrangements for the one-year PO follow-up visit.
Working length, apical size, and obturation technique
| Canal | Working Length | Apical Size | Obturation Materials and Techniques |
| MB | 18.0 mm | 30 | AH26® sealer, Lateral condensation |
| ML | 18.0 mm | 30 | AH26® sealer, Lateral condensation |
D canal was not treated

Figure 18.7 Working radiograph monitoring the obturation process.

Figure 18.8 Final radiograph taken after obturation of root canal space and restoration of endodontic access.
Post-Treatment Evaluation
Third visit (1-year follow-up): The Pt presented with symptoms of mild discomfort on the right side of the face. She pointed to the region of the right buccinator and masseter muscles. There was no visible facial swelling or submandibular lymphadenopathy. Nevertheless, the muscles were tender on palpation. Tooth #31 was negative for percussion and palpation sensitivity. There was no swelling in the adjacent gingival tissue. The condition of tooth #31 was determined to be stable. The Pt was reassured of no recurrence of periapical infection and informed that the symptoms might indicate possible bruxism or clenching habit. One-year follow-up 2-D periapical radiograph indicated complete resolution of the periapical lesion (Figure 18.9).
Fourth visit (2-year follow-up): The Pt reported no symptoms associated with tooth #31. The crown and the amalgam restoration in the endodontic access were intact. Tooth #31 showed no signs of sensitivity to percussion and palpation. The right buccinator and masseter muscles were not tender on palpation. There was no swelling in the adjacent gingival tissue. Probing depth was less than 3 mm including the furcation area revealed complete healing of the previous radiolucency with uniform PDL and sclerosis of the periapical bone. The follow-up 3-D CBCT image (Figure 18.10) also revealed complete osseous healing of the periapical tissue of tooth #31. The periapical tissue of the D root was also intact in both imaging modalities.

Figure 18.9 One-year follow-up 2-D radiograph indicating complete resolution of the periapical lesion.

Figure 18.10 Comparison of 3-D CBCT images taken preoperatively (top) and at 1-year follow-up (bottom) showing complete osseous healing of the periapical lesion.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


