Introduction
The aim of this research was to compare maxillary and mandibular molar heights and incisor inclinations in patients with skeletal open-bite Class II, patients with skeletal open-bite Class III, and an untreated control group.
Methods
Pretreatment lateral cephalograms of 70 orthodontic patients (34 men, 36 women) between 16 and 40 years of age were examined. The sample was divided into 3 groups according to facial growth pattern and overbite. The control group (n = 25) included normodivergent Class I subjects with adequate overbite; the skeletal open-bite Class II group (n = 25) and the skeletal open-bite Class III group (n = 20) included hyperdivergent Class II or Class III subjects with negative overbite. Measurements considered were ANB angle, palatal and mandibular plane angles, maxillary incisor palatal plane angulation, and mandibular incisor mandibular plane angulation, as well as the distance from the palatal or the mandibular plane to the mesial cusp of the molars. Multivariate analysis of covariance and multivariate analysis of variance tests were used to determine the differences between the groups, followed by the Tukey post-hoc test. Additionally, the Mann-Whitney U test and Kruskall-Wallis test were performed.
Results
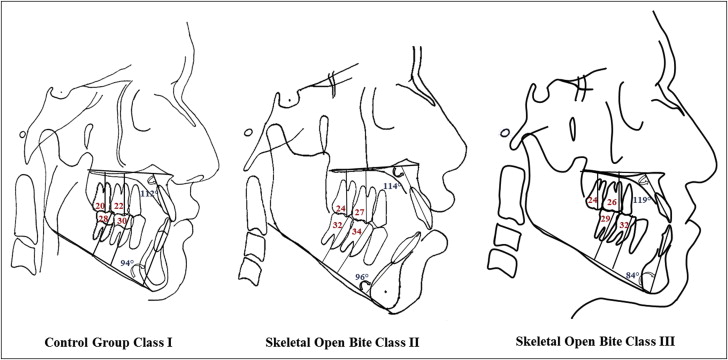
Significant differences in molar height were found ( P <0.001). A 4-mm difference in maxillary molar height between the skeletal open-bite and control groups was found. Mandibular molar height was greater in the skeletal open-bite Class II group ( P <0.001). Maxillary incisor palatal plane angulation was greater in the skeletal open-bite Class III group by approximately 6°. Mandibular incisor to mandibular plane angulation was 10° more lingual in the skeletal open-bite Class III group ( P <0.001).
Conclusions
The skeletal open-bite groups had greater molar heights than did the control group. The skeletal open-bite Class II group had more eruption of the mandibular molars. The maxillary incisors were more proclined and the mandibular incisors were more lingual in the skeletal open-bite Class III group.
An anterior open bite is considered to be one of the most difficult problems to treat in orthodontics. Prevalences of 3.5% to 16.5% have been reported. Various treatment modalities for the correction of an anterior open bite have been proposed, such as orthognathic surgery and orthodontic camouflage treatment. Among the nonsurgical options, when the intrusion of molars is a treatment goal, several therapeutic options have been proposed, such as multiloop edgewise archwires, microimplants, and microplates. Another suggested treatment alternative is extrusion of the anterior teeth after careful consideration of the implications of smile esthetics.
Skeletal open bite mostly involves a negative overbite, hyperdivergence of the mandibular and palatal planes, excessive clockwise facial growth, augmented anterior facial height, and proclined incisors. In addition, the 2 occlusal planes at different levels have been noted—an anterior level that includes the canines and incisors tilted up, and a posterior level tilted downward with the molars and premolars almost always extruded. The greater molar height might result from the lack of space in the dental arch for complete third molar eruption with associated anterior pressure on the second molars that can cause tooth crowding and eruption. This concept is known as a posterior discrepancy. Open bites are relatively common in patients with skeletal Class II and Class III malocclusions (Ruíz et al, unpublished data). In the case of a skeletal Class III open bite, maxillary retrusion is common, whereas in skeletal Class II patients, mandibular retrusion is more frequent.
The importance of molar height and incisor inclination with respect to mandibular plane variation has been recognized. Molar height can be influenced by different facial growth types and directions. Ruíz et al (unpublished data) found no significant differences in maxillary molar height according to the vertical or horizontal pattern. However, they did not analyze open-bite patients; they considered only subjects with adequate overbite. In contrast, Kucera et al concluded that increased molar height is a common finding in adults with skeletal open bite, but they did not distinguish whether their subjects were Class II or Class III, and where specifically the alteration was located. They suggested that orthodontic treatments for these patients should be aimed primarily at limiting or correcting the excessive dentoalveolar eruption in the maxillary and mandibular posterior regions. With respect to incisor inclinations, significant differences have been found in open-bite and control groups.
Therefore, the purpose of this study was to compare the heights of the maxillary and mandibular first and second molars and the inclinations of the maxillary and mandibular incisors in Class II and Class III skeletal open-bite patients and compare them with a control group with normal skeletal features. This information will fill a current knowledge gap in regard to the relative contribution of vertical and sagittal dental positional contributions in skeletal open-bite patients from different sagittal skeletal origins.
Material and methods
The sample included 70 pretreatment lateral cephalograms (34 men, 36 women) in maximum intercuspation imaged at a radiologic diagnostic center in Lima, Perú. Subjects receiving orthodontic treatment at the time of acquisition were not considered. Their age range was 16 to 40 years (all were in cervical vertebral stage 6 ). The study was approved by the local ethics committee. Sample size was calculated by considering a mean difference of 2.5 mm as a clinically relevant difference between study groups (obtained from a preliminary pilot study in which the means of the maxillary molar heights between the open-bite Class II and the control subjects were compared) and a standard deviation of 2 mm. With a 1-sided significance level of 0.05 and a power of 80%, a minimum of 8 patients per skeletal group were required.
Imaging was performed with digital cephalometric panoramic equipment (ProMax; Planmeca, Helsinki, Finland). Device settings were 16 mA, 72 kV, and 9.9 seconds. Cephalometric analyses were performed with MicroDicom viewer software (version 0.8.1; Simeon Antonov Stoykov, Sofia, Bulgaria), without magnification, at a scale of 1:1.
The definitions of the cephalometric points and angles used in this study were those described by Riolo et al, Kucera et al, and Burstone et al ( Table I ).
| Angular measurements (°) | Definition |
|---|---|
| ANB | The angle between points A and B |
| SN-MP | The angle between the nasion-sella plane and the mandibular plane |
| PP-MP | The angle between the palatal plane and the mandibular plane |
| UIPP | The angle between the maxillary incisor inclination and the palatal plane |
| LIMP | The angle between the mandibular incisor inclination and the mandibular plane |
| Linear measurements (mm) | |
|---|---|
| Maxillary first molar height | The length of a line perpendicular to the palatal plane extending from the palatal plane to the mesial cusp tip of the maxillary first molar |
| Maxillary second molar height | The length of a line perpendicular to the palatal plane extending from the palatal plane to the mesial cusp tip of the maxillary second molar |
| Mandibular first molar height | The length of a line perpendicular to the mandibular line extending from the mandibular line to the mesial cusp tip of the mandibular first molar |
| Mandibular second molar height | The length of a line perpendicular to the mandibular line extending from the mandibular line to the mesial cusp tip of the mandibular second molar |
The study sample comprised 3 groups categorized according to their facial growth patterns and overbites ( Tables II and III ).
| Group | Measurement | n | Mean (°) | SD (°) | Minimum (°) | Maximum (°) | P |
|---|---|---|---|---|---|---|---|
| 1. Class I (control) | Age | 25 | 22.60 | 4.77 | 17.00 | 35.00 | 0.084 ∗ |
| ANB angle | 25 | 2.91 | 0.94 | 0.57 | 4.50 | <0.001 ∗ † | |
| NS-ML angle | 25 | 32.21 | 2.43 | 27.00 | 37.00 | <0.001 ∗ † | |
| PP-MP angle | 25 | 24.80 | 2.48 | 23.00 | 29.00 | <0.001 ∗ † | |
| 2. Skeletal open-bite Class II | Age | 25 | 23.24 | 9.68 | 16.00 | 40.00 | |
| ANB angle | 25 | 6.74 | 1.45 | 5.00 | 10.11 | ||
| NS-ML angle | 25 | 44.09 | 3.80 | 40.01 | 52.00 | ||
| PP-MP angle | 25 | 33.65 | 3.32 | 30.00 | 37.60 | ||
| 3. Skeletal open-bite Class III | Age | 20 | 20.00 | 3.96 | 16.00 | 27.00 | |
| ANB angle | 20 | −0.88 | 0.82 | −0.10 | −2.60 | ||
| NS-ML angle | 20 | 42.51 | 2.33 | 40.00 | 47.29 | ||
| PP-MP angle | 20 | 32.65 | 2.15 | 30.00 | 35.76 |
† Tukey test: ANB: ( P <0.001, 1 and 2) ( P <0.001, 1 and 3) ( P <0.001, 2 and 3); NS-ML: ( P <0.001, 1 and 2) ( P <0.001, 1 and 3) ( P = 0.341, 2 and 3); PP-MP: ( P <0.001, 1 and 2) ( P = 0.001, 1 and 3) ( P = 0.800, 2 and 3).
| Group | Sex | Total (n) | |
|---|---|---|---|
| Female (n) | Male (n) | ||
| Class I (control) | 12 | 13 | 25 |
| Skeletal open-bite Class II | 14 | 11 | 25 |
| Skeletal open-bite Class III | 10 | 10 | 20 |
| Total | 36 | 34 | 70 |
The control group (n = 25; mean age, 22.6 years) included subjects who met the following criteria: ANB 2° ± 2°, bilateral Angle Class I occlusion, bilateral Class I molar relationship, mandibular plane angle in the range of 33° ± 6°, palatal plane to mandibular plane angle of 26° ± 3°, overjet between 2 and 3 mm, overbite between 1 and 4 mm, and complete permanent dentition (including third molars).
The skeletal open-bite Class II group (n = 25; mean age, 23.4 years) included subjects who met the following criteria: ANB greater than 5°, Angle Class II Division 1 malocclusion, bilateral Class II molar relationship, overjet greater than 5 mm, mandibular plane angle greater than 40°, hyperdivergent palatal plane angle (>29°), negative overbite greater than 0.5 mm, and complete permanent dentition (including third molars).
The skeletal open-bite Class III group (n = 20; mean age, 20 years) included subjects who met the following criteria: ANB less than 0°, Angle Class III malocclusion, bilateral Class III molar relationship, overjet smaller than −1 mm, mandibular plane angle greater than 40°, hyperdivergent palatal plane angle (>29°), negative overbite greater than 0.5 mm, and complete permanent dentition (including third molars).
Molar height ( Fig 1 ) was defined as the length of a line perpendicular to the palatal plane extending from the palatal plane to the mesial cusp tip at the occlusal plane for each maxillary molar. For the mandibular molars, the length of a line perpendicular to the mandibular line extending from the mandibular line to the mesial cusp tip at the occlusal plane of each mandibular molar was evaluated.
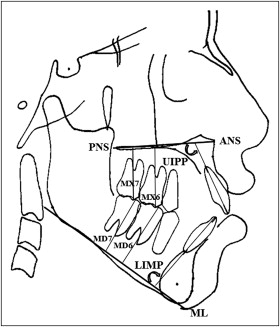
Maxillary incisor inclination was evaluated by considering the angle formed between the palatal plane and the long axis of the maxillary central incisor, and the mandibular incisor inclination by the angle formed by the mandibular plane and the mandibular central incisor’s long axis ( Fig 1 ).
Statistical analysis
All statistical analyses were performed using SPSS software for Windows (version 20; IBM SPSS, Chicago, Ill). Statistical significance was set at P <0.05 for all the tests. Descriptive data were reported as means and standard deviations.
A multivariate analysis of covariance test was used to assess the influence of age, sex, group, and their interactions on molar height and incisor inclination. Due to the lack of significance of age, multivariate analysis of variance (MANOVA) was done without age as a covariate, and 1-way analysis of variance (ANOVA) was performed to determine whether there were differences in the 3 groups between molar height and incisor inclination. If normality and homogeneity of variance assumptions were satisfied, the Tukey honestly significant difference post-hoc test was used for multiple comparisons.
Only when the normality and homogeneity of variance assumptions were not satisfied, we used a nonparametric Kruskal-Wallis H test. Also, the Mann-Whitney U test was used to determine where the differences were specifically. Statistical significance was set at P <0.05 for all tests.
Results
The intraexaminer reliability was assessed with the intraclass correlation coefficient, which gave a result greater than 0.90 for all measurements. In addition, the Dahlberg errors were less than 1 mm for linear measurements and 0.3° for angular measurements ( Table IV ). All cephalometric tracings were made with a 2-month interval between them.
| Measurement | Intraobserver concordance | Dahlberg error S X = Σ D 2 2 N | ||
|---|---|---|---|---|
| ICC | CI inferior limit | CI superior limit | ||
| Maxillary first molar height | 0.990 | 0.930 | 0.999 | 0.8 mm |
| Maxillary second molar height | 0.985 | 0.930 | 0.998 | 1 mm |
| Mandibular first molar height | 0.983 | 0.900 | 0.999 | 0.9 mm |
| Mandibular second molar height | 0.901 | 0.900 | 0.965 | 0.5 mm |
| UIPP | 0.990 | 0.995 | 0.999 | 0.3° |
| LIMP | 0.950 | 0.920 | 0.990 | 0.3° |
Distribution of the sample by facial growth pattern and sex is given in Table III .
A MANOVA test assessing molar height and incisor inclination based on group, sex, and their interactions is presented in Table V . The group and sex interaction was not significant except for the mandibular incisor to mandibular plane angle. Sex was significant only for molar height but not for incisor inclination.
| Dependent variable | Covariables and fixed factors | P |
|---|---|---|
| Maxillary first molar height | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | <0.001 | |
| Group∗sex | 0.334 | |
| Maxillary second molar height | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | <0.001 | |
| Group∗sex | 0.727 | |
| Mandibular first molar height | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | <0.001 | |
| Group∗sex | 0.500 | |
| Mandibular second molar height | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | <0.001 | |
| Group∗sex | 0.431 | |
| UIPP | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | 0.649 | |
| Group∗sex | 0.075 | |
| LIMP | Corrected model | <0.001 |
| Intercept | <0.001 | |
| Group | <0.001 | |
| Sex | 0.808 | |
| Group∗sex | 0.003 |
For molar height ( Fig 2 ), there was a statistically significant difference ( P <0.001) of about 4.5 mm at the maxillary first molar height between the skeletal open-bite groups (Class II, 26.64 mm; Class III, 26.06 mm) and the control group (22.02 mm) ( Table VI ).
| Measurement | Group | n | Mean (°) | SD (°) | Minimum (°) | Maximum (°) | S 2 | P |
|---|---|---|---|---|---|---|---|---|
| Maxillary first molar height | 1. Class I (control) | 25 | 22.02 | 1.75 | 19.70 | 26.10 | 3.06 | <0.001 ∗ † |
| 2. Skeletal open-bite Class II | 25 | 26.64 | 2.73 | 22.36 | 34.20 | 7.46 | ||
| 3. Skeletal open-bite Class III | 20 | 26.06 | 1.83 | 23.00 | 29.00 | 3.35 | ||
| Maxillary second molar height | 1. Class I (control) | 25 | 19.65 | 2.38 | 15.76 | 25.00 | 5.66 | <0.001 ∗ † |
| 2. Skeletal open-bite Class II | 25 | 23.69 | 2.80 | 19.26 | 31.57 | 7.84 | ||
| 3. Skeletal open-bite Class III | 20 | 23.95 | 2.40 | 20.00 | 27.22 | 5.76 | ||
| Mandibular first molar height | 1. Class I (control) | 25 | 29.68 | 2.30 | 25.70 | 34.00 | 5.30 | <0.001 ∗ † |
| 2. Skeletal open-bite Class II | 25 | 34.16 | 3.66 | 28.00 | 40.26 | 13.42 | ||
| 3. Skeletal open-bite Class III | 20 | 31.64 | 2.96 | 24.40 | 36.12 | 8.80 | ||
| Mandibular second molar height | 1. Class I (control) | 25 | 28.32 | 2.09 | 25.00 | 32.15 | 4.40 | <0.001 ∗ † |
| 2. Skeletal open-bite Class II | 25 | 31.65 | 3.42 | 26.25 | 38.24 | 11.72 | ||
| 3. Skeletal open-bite Class III | 20 | 28.70 | 2.47 | 22.30 | 32.00 | 6.13 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


