Introduction
In this study, we aimed to measure the inclination of teeth on dental casts by a manual technique with the tooth inclination protractor (TIP; MBI, Newport, United Kingdom) and a newly designed 3-dimensional (3D) software program. The correlation of the 2 techniques was evaluated, and the reliability of each technique was assessed separately.
Methods
This study was conducted on 36 dental casts of normal, well-aligned Class I occlusions; we assessed 432 teeth. All casts had a normal Class I occlusion. After determining the facial axis of the clinical crown and the facial axis points on the dental casts, we measured the inclinations of the incisors and posterior teeth up to the first molars in each dental arch relative to Andrews’ occlusal plane and the posterior occlusal plane using the TIP. Moreover, the casts were scanned by a structured-light 3D scanner. The inclination of teeth relative to the occlusal plane was determined using the new software. To assess the reliability, measurements of all teeth from 15 casts were repeated twice by the 2 methods. Intraclass correlation coefficient and Dahlberg’s formula were used for calculation of correlation and reliability.
Results
Overall, the 2 techniques were not significantly different in the measurements of the inclinations of the teeth in both jaws. The ranges of Dahlberg’s formula were 3.1° to 5.8° for the maxilla and 3.3° to 5.9° for the mandible. The overall correlation of the 2 techniques according to the intraclass correlation coefficient was 0.91. For calculation of reliability, the intraclass correlation coefficients for the TIP and the 3D method were 0.73 and 0.82, respectively.
Conclusions
The TIP and the 3D software showed a high correlation for measurement of the inclinations of maxillary and mandibular teeth relative to the occlusal plane. Also, the reproducibility of the measurements in each method was high.
Highlights
- •
We compared the TIP and a 3D software for measuring the inclinations of the teeth.
- •
The inclinations of the teeth in each dental arch were measured by the TIP on casts.
- •
The inclinations of the teeth were measured on 3D scans by the software.
- •
The TIP and the 3D software showed a high correlation for measurement of the inclinations.
- •
The reproducibility of measurements in each method was high.
The inclination of anterior teeth is an extremely important factor in smile esthetics. It has been introduced as 1 of the 6 keys of occlusion by Andrews. Moreover, it is a fundamental parameter in determination of the prescription of preadjusted orthodontic appliances. Two issues are important for the measurement of tooth inclination: the measurement tool and the defined landmarks. Several tools have been used for this purpose: cephalometric angular measurements, conveyor and compass on dental casts, the tooth inclination protractor (TIP; MBI, Newport, United Kingdom) on the casts or intraorally, and 3-dimensional (3D) methods including angular measurements on 3D cast models or cone-beam computed tomography (CBCT). An accurate error-free technique for this purpose has yet to be found. However, the TIP has been demonstrated to be an inexpensive, easy-to-use, noninvasive, and reliable method for measuring incisor crown inclination. Moreover, 3D techniques have high reliability and accuracy for such angular measurements.
Landmarks used for measuring tooth inclinations are different in lateral cephalograms, cast measurements, 3D models, and 3D imaging (CBCT). In 2-dimensional and 3D radiographic techniques, the long axis of the tooth has been used ; in cast-based or intraoral measurements, the facial axis of the clinical crown has been used. Moreover, different horizontal reference planes have been used in various studies. Cephalometric methods use palatal, mandibular, and occlusal reference planes. Andrews used an occlusal plane that was approximated with a plastic template. This template was in contact with the anterior and posterior teeth. He used this method for measuring tooth inclination represented by tip and torque. Ross et al introduced the posterior occlusal plane for measuring the inclination of posterior teeth. This plane was tangent with the most occlusal cusp points in both first molars, and 1 or 2 premolars. Richmond et al used their own invented device, the TIP, with an occlusal plane similar to that of Andrews. In the 3D cast-based methods and radiography, different reference planes have been used. Overall, changes in the horizontal reference plane compromise the validity of different methods for measuring tooth inclinations (relative to one another, or at different treatment phases). However, this plane might have a minimal impact on reliability.
At present, modern 3D digital technologies make such measurements easily possible in a short time and with high accuracy. Furthermore, software programs have been developed for 3D analysis of dental casts used for diagnosis of discrepancies, treatment planning, and evaluation of changes as a result of treatment. These software programs have the potential for measuring all 6 keys of ideal occlusion suggested by Andrews. Several manufacturers, such as Orthocad, Orthoproof, and O3DM, have introduced commercial software programs for analyzing digital models and measuring linear and angular parameters on 3D models.
Considering all the above, in this study we had the following objectives: (1) to measure the inclinations of the incisors, canines, premolars, and first molars on dental casts using the TIP and a 3D software developed at Shahid Beheshti Dental School in Tehran, Iran; (2) to assess the correlations of the 2 techniques and the discrepancies between measurements; and (3) to assess the reliability of the 2 techniques.
The null hypothesis of the study was that no significant correlation exists between measurements made with the TIP and the computer software.
Material and methods
This study was conducted on 36 dental casts of normal and well-aligned Class I occlusions (432 teeth). The buccolingual inclinations of the incisors, canines, premolars, and first molars (12 teeth in each cast) were measured by the TIP and a 3D laser scanner. These normal-occlusion casts were selected from the cast archives of Qazvin Dental School in Qazvin, Iran, using convenience sampling.
We used the following tools. The TIP was used to measure the inclinations of the anterior teeth, premolars, and molars on the dental casts and in the mouth: this device has a horizontal plane, a conveyor, and a rod for contact with the labial surfaces of the teeth for measuring the axial inclination of the tooth crown. A structured-light 3D scanner (Maestro3D Desktop Scanner; AGE Solutions, Pontedera, Italy) was used for the 3D scanning of the dental casts with 10-μm readability.
The measurement technique was the following. First, the locations of the facial axis points were marked on each tooth with a fine-tip pencil (diameter, 0.5 mm) according to the method of Andrews.
For measuring the inclinations of the anterior teeth with the TIP, the horizontal plane of the device was placed in contact with the occlusal plane, as described by Andrews. Then, the axial inclination of the crown was recorded by contacting the vertical rod with the crown surface and reading the degree displayed by the conveyor ( Fig 1 , A and B ).
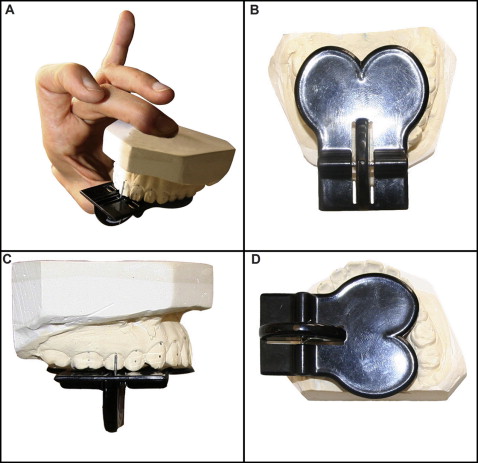
For measuring the inclinations of the canines, premolars, and first molars, the posterior occlusal plane was used as described by Ross et al, and the axial inclination of teeth was measured as described for the anterior teeth. Because of the TIP’s structure, using the occlusal plane, including the contact points with all incisors, was not possible in all cases when measuring the inclinations of the canines, premolars, and molars ( Fig 1 , C and D ).
For the 3D measurements, all casts were digitized by the 3D scanner, and their 3D models were saved in stereolithography format.
A simulator software program for 3D measurement was developed at the Orthodontic Department of Shahid Beheshti Dental School in Iran by 1 of the authors (A.H.A.), a dentist who also has a master’s degree in computer science (artificial intelligence). This software has the following capabilities: display of 3D point clouds, triangulation of the point cloud and production of the object’s surface, measurement of distances between points in a virtual model, definition of occlusal and sagittal planes, measurement of the inclination of each tooth, and superimposition of 2 dental models based on the marked reference points. The software was developed using the C.Net format ( Fig 2 , A ).
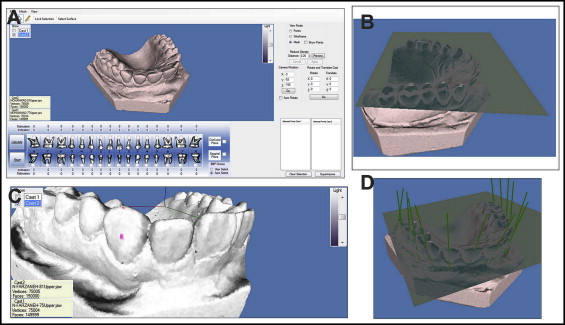
To determine the horizontal reference plane, the cast file was opened in the software, and the occlusal plane was drawn according to the method of Sjogren et al, using the incisal edge of a central incisor and the mesiobuccal cusp tips of the maxillary first molars (3 points), and the incisal edge of a central incisor and the mesiobuccal cusp tips of the mandibular second molars (3 points) ( Fig 2 , B ).
In the next phase, the respective tooth was selected, and its facial axis point was marked automatically as the midpoint between 2 points: the midpoint of the buccal side of the occlusal table or incisal edge, and the deepest point on the cementoenamel junction. Then the software drew a tangent line to the facial axis point using these data and reported its angle relative to the occlusal plane as the inclination value. This was performed separately for all teeth in all dental casts ( Fig 2 , C and D ).
Because the reading accuracy of the 2 devices was not similar, the measurements made by the 3D method were rounded to 1° to be comparable with the TIP method. To assess the correlation between the 2 methods, the torque measured by the TIP was compared with the corresponding value measured by the software with intraclass correlation coefficients (ICCs). Also, the differences between measurements were calculated using the Dahlberg index. For assessing reliability, the measurements in each method were repeated twice on 15 casts with a 1-week interval, and the ICC and the Dahlberg index were calculated. The null hypothesis of the study was that no significant correlation exists between measurements made with the TIP and the computer software. Thus, P <0.05 indicated no significant difference between the 2 measurement techniques.
Results
We determined the correlations of the 2 methods and the differences between them. Table I indicates the mean torque for the maxillary teeth measured by the 2 methods, its standard deviations, results of the F test, the P values, the ICC, and the Dahlberg index when comparing the methods. The same data for the mandibular teeth are shown in Table II . In the maxilla, the 2 methods had acceptable correlations ( P <0.05) for all teeth. Also, according to the Dahlberg index, the differences in measurements ranged from 3.1° (left central incisor) to 5.8° (left lateral incisor).
| Tooth | Maxillary right | Maxillary left | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | |
| 3D | ||||||||||||
| Mean | −10.5 | −10.9 | −7.5 | −4.8 | 10.6 | 10.5 | 8.6 | 8.2 | −5.9 | −8.8 | −12.9 | −9.8 |
| SD | 4.8 | 6.4 | 7.6 | 7.4 | 5.7 | 6.1 | 4.4 | 7.6 | 5.7 | 8.5 | 7.6 | 3.5 |
| TIP | ||||||||||||
| Mean | −11.1 | −13.7 | −11.8 | −5.4 | 8.2 | 7.1 | 6.7 | 4.4 | −6.6 | −12.4 | −14.1 | −10.9 |
| SD | 6.7 | 5.1 | 4.2 | 5.7 | 4.1 | 6.2 | 6.0 | 5.9 | 4.7 | 5.7 | 7.3 | 6.3 |
| F | 3.547 | 5.376 | 2.320 | 5.692 | 3.049 | 3.900 | 5.548 | 2.227 | 3.141 | 2.973 | 4.446 | 3.501 |
| P value | 0.006 | 0.001 | 0.046 | 0.000 | 0.014 | 0.004 | 0.000 | 0.054 | 0.012 | 0.015 | 0.002 | 0.007 |
| ICC (r) | 0.727 | 0.771 | 0.492 | 0.830 | 0.636 | 0.689 | 0.796 | 0.507 | 0.690 | 0.622 | 0.779 | 0.721 |
| Dahlberg | 3.8 | 3.7 | 5.6 | 3.5 | 3.8 | 4.5 | 3.1 | 5.8 | 3.6 | 5.6 | 4.5 | 4.5 |
| Tooth | Mandibular right | Mandibular left | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | |
| 3D | ||||||||||||
| Mean | −36.1 | −25.4 | −18.2 | −10.3 | 1.8 | 7.9 | 6.4 | 3.6 | −9.2 | −21 | −27.4 | −32.9 |
| SD | 4.9 | 7.5 | 6.9 | 6.0 | 8.0 | 8.0 | 7.7 | 7.8 | 7.7 | 6.4 | 8.9 | 5.8 |
| TIP | ||||||||||||
| Mean | −35.3 | −24.9 | −20.3 | −11.5 | 0.7 | 3.9 | 3.2 | 0.2 | −11.3 | −23.1 | −28.2 | −33.4 |
| SD | 5.8 | 6.5 | 6.0 | 6.9 | 5.7 | 6.2 | 6.7 | 6.3 | 7.7 | 8.9 | 7.1 | 6.1 |
| F | 5.585 | 2.633 | 2.045 | 6.739 | 5.971 | 10.405 | 4.035 | 7.934 | 8.754 | 2.470 | 6.031 | 3.603 |
| P value | 0.001 | 0.027 | 0.075 | 0.000 | 0.000 | 0.000 | 0.003 | 0.000 | 0.000 | 0.035 | 0.000 | 0.009 |
| ICC (r) | 0.757 | 0.633 | 0.505 | 0.850 | 0.835 | 0.843 | 0.719 | 0.827 | 0.873 | 0.593 | 0.839 | 0.734 |
| Dahlberg | 3.6 | 5.1 | 5.3 | 3.3 | 3.7 | 4.1 | 4.9 | 4 | 3.7 | 5.9 | 4.2 | 3.8 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


