Mandibular Vestibular Approach
The mandibular vestibular approach is useful in a wide variety of procedures. It allows relatively safe access to the entire facial surface of the mandibular skeleton, from the condyle to the symphysis. One advantage of this approach is the ability to constantly assess the dental occlusion during surgery. The greatest benefit to the patient is the hidden intraoral scar. The approach is also relatively rapid and simple, although access is limited in some regions, such as the lower border of the mandible at the angle and parts of the ramus. Complications are few but include mental nerve damage and lip malposition, both of which are minimized with the use of proper technique.
SURGICAL ANATOMY
Mental Nerve
The only neurovascular structure of any significance that must be negotiated during procedures in the mandibular body/symphysis region is the mental neurovascular bundle. The artery and vein that accompany the mental nerve are insignificant from a surgical standpoint. The mental nerve is a terminal branch of the inferior alveolar nerve (mandibular nerve), and is sensory to the skin and mucosa of the lower lip, the skin in the region of the chin, and the facial gingiva of the anterior teeth.
The mental nerve exits the mental foramen that is located midway between the alveolar and basal borders of the mandible and is usually below or slightly anterior to the second bicuspid tooth (see Fig. 8.1). The mental nerve divides under the depressor anguli oris muscle into three main branches; one descends to the skin of the chin and the other two ascend to the skin and mucous membrane of the lower lip and gingiva. The branching pattern is variable however, and several finer branches may be noted. As the branches enter the lower lip, they become superficial and can usually be seen just beneath the mucosa of the lower lip when it is everted.
Facial Vessels
The facial artery and vein are usually not encountered during the mandibular vestibular approach unless dissection through the periosteum occurs in the region of the mandibular antegonial notch.
The facial artery arises from the external carotid artery in the carotid triangle of the neck. At or close to its origin, it is crossed by the posterior belly of the digastric muscle, the stylohyoid muscles, and the hypoglossal nerve. In the submandibular triangle, the facial
artery ascends deep to the submandibular gland, grooving its deep and superior aspect, and then passes superficially to reach the inferior border of the mandible. As the artery crosses the mandible at the anterior border of the masseter muscle, it is covered on its superficial surface by skin and platysma muscle, and its pulsations can be felt at this location.
artery ascends deep to the submandibular gland, grooving its deep and superior aspect, and then passes superficially to reach the inferior border of the mandible. As the artery crosses the mandible at the anterior border of the masseter muscle, it is covered on its superficial surface by skin and platysma muscle, and its pulsations can be felt at this location.
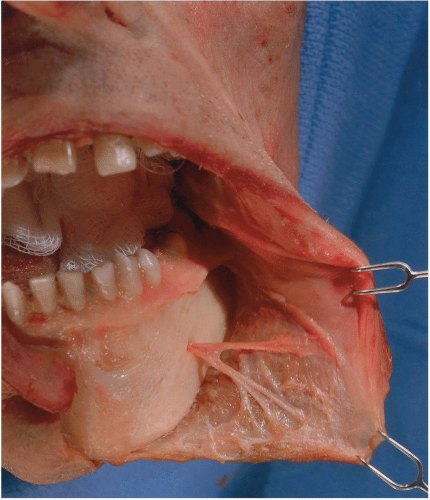
Figure 8.1 Anatomic dissection of mental nerve branches.
|
The facial vein is the drainage of the angular and ultimately labial vessels. It is usually located more posterior and superficial to the artery. Of surgical significance, however, is the fact that the facial artery and vein are close to the mandible in the region of the inferior border. The only structure that separates the vessels from the bone is the periosteum (see Fig. 8.2).
Mentalis Muscle
The only muscle of facial expression that is important from a surgical standpoint when using the mandibular vestibular approach is the mentalis muscle. All the other muscles of facial expression are stripped from the mandible by subperiosteal dissection and are readily reattached with soft tissue closure. The mentalis muscle is unique however, in that it is the only elevator of the lower lip and chin. If this muscle is not properly repositioned during closure, the chin will “droop” and the lower lip will take on a lifeless, sagging appearance, exposing more lower teeth.
The mentalis muscles are paired, small, conical muscles arising from the mandible, beginning at the midroot level of the lower incisor teeth and continuing inferiorly to a point below the apices. The muscles are separated from one another by a firm septum and adipose tissue (see Fig. 8.3).
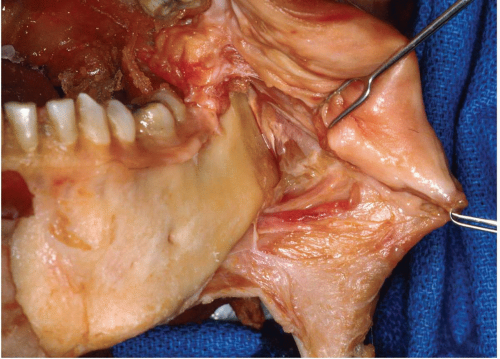
Figure 8.2 Anatomic dissection of the mandibular body showing relation of facial vessels to bone. The only tissue between them is the periosteum.
|
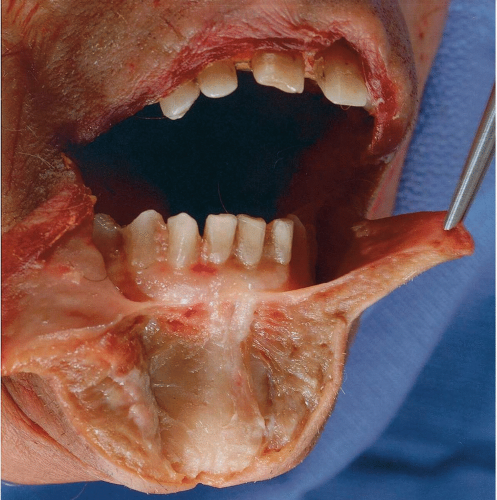
Figure 8.3 Anatomic dissection showing cross section of soft tissues of the chin. Note the direction of the mentalis muscle fibers.
|
At the inferior portion of its origin, the mentalis muscle attaches lateral to the mental trigone. The fibers of this muscle pass from their origin inferiorly, inserting into the skin of the chin at the soft tissue chin prominence. The most superior fibers are the shortest and pass almost horizontally into the skin of the upper chin. The lower fibers are the longest and pass obliquely or vertically to the skin at the lower part of the chin. The origin of the mentalis muscle determines the depth of the labial sulcus in the anterior portion of the mouth. The mentalis muscle is innervated by the marginal mandibular branch of the facial nerve.
Buccal Fat Pad
The buccal fat pad consists of a main body and four extensions: buccal, pterygoid, pterygomandibular, and temporal. The body is centrally positioned. The buccal extension lies superficially within the cheek, while the pterygoid, pterygomandibular, and temporal extensions are more deeply situated.
The buccal extension is the most superficial segment of the fat pad and imparts fullness to the cheek. It enters the cheek below the parotid duct and extends along the anterior border of the masseter as it descends into the mandibular retromolar region. It overlies the main portion of the buccinator muscle as it crosses the cheek. In the cheek, the fat pad is anterior to the ramus. Its caudal extension intraorally is on a plane tangential with the occlusal surface of the mandibular third molar (see Fig. 8.4). Its anterior limit is marked by
the facial vessels, which are in the same plane as the buccal fat pad. The parotid duct lies superficial to the fat pad and then penetrates the fat pad and buccinator to enter the oral cavity opposite the second molar. The buccal extension of the fat pad is limited by the masseteric fascia. A deep extension of the masseteric fascia blends with the fascia along the lateral surface of the buccinator. This fascial layer lines the deep surface of the buccal fat that is in contact with the buccinator.
the facial vessels, which are in the same plane as the buccal fat pad. The parotid duct lies superficial to the fat pad and then penetrates the fat pad and buccinator to enter the oral cavity opposite the second molar. The buccal extension of the fat pad is limited by the masseteric fascia. A deep extension of the masseteric fascia blends with the fascia along the lateral surface of the buccinator. This fascial layer lines the deep surface of the buccal fat that is in contact with the buccinator.
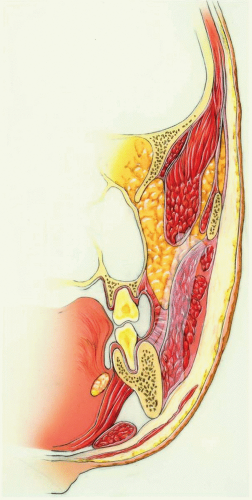
Figure 8.4 Relation between the buccal fat pad and the retromolar region. Note that the fat extends inferiorly to just above the occlusal plane. Incisions made through the buccinator muscle superior to the occlusal plane will cause entry into the fat pad.
|
TECHNIQUE
For demonstration purposes, the technique subsequently described is that used to expose the entire facial surface of the mandible. The length of the incision and the extent of subperiosteal dissection, however, depend on the area of interest and the extent of surgical intervention. While the vestibular approach is used for patients who have teeth, when large segments of teeth are absent the surgeon should consider incisions along the alveolar crest as opposed to vestibular ones.
▶ Step 1. Injection of Vasoconstrictor
The oral mucosa, submucosa, and facial muscles are lushly vascularized. Submucosal injection of a vasoconstrictor can remarkably reduce the amount of hemorrhage during incision and dissection.
▶ Step 2. Incision
In the anterior region, from canine to canine, the lower lip is everted and a scalpel or electrocautery is used to incise mucosa. The incision is curvilinear, extending anteriorly out into the lip, leaving 10 to 15 mm of mucosa attached to the gingiva (see Fig. 8.5). It is
important to incise only through the mucosa because mental nerve branches that extend into the upper lip are often seen just below the mucosa (see Fig. 8.6). Once through the mucosa, the underlying mentalis muscles are clearly visible. The muscle fibers are sharply incised in an oblique approach to the mandible (see Fig. 8.7). It is important to avoid the mental nerve during the incision. The incision should therefore be made more superiorly in the canine and premolar region (see Fig. 8.8). Any incision placed more inferior in the canine/premolar region may sever branches of the mental nerve. The scalpel should therefore be oriented perpendicular to the bone when incising above the mental foramen to prevent incision of this nerve. When bone is encountered, there should be an ample amount of mentalis muscle remaining on its origin for holding deep sutures at closure (see Fig. 8.9).
important to incise only through the mucosa because mental nerve branches that extend into the upper lip are often seen just below the mucosa (see Fig. 8.6). Once through the mucosa, the underlying mentalis muscles are clearly visible. The muscle fibers are sharply incised in an oblique approach to the mandible (see Fig. 8.7). It is important to avoid the mental nerve during the incision. The incision should therefore be made more superiorly in the canine and premolar region (see Fig. 8.8). Any incision placed more inferior in the canine/premolar region may sever branches of the mental nerve. The scalpel should therefore be oriented perpendicular to the bone when incising above the mental foramen to prevent incision of this nerve. When bone is encountered, there should be an ample amount of mentalis muscle remaining on its origin for holding deep sutures at closure (see Fig. 8.9).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


