The Tweed-Merrifield directional force technique is a useful treatment approach for a patient with a Class II malocclusion with dentoalveolar protrusion. The purpose of this case report was to present the diagnosis and treatment descriptions of a patient with an Angle Class II malocclusion complicated by tooth losses, severe dentoalveolar protrusion, and skeletal discrepancy. Treatment involved extraction of the maxillary first premolars, high-pull headgear to enhance anchorage, and high-pull J-hook headgear to retract and intrude the maxillary anterior segments. A successful outcome was achieved with traditional orthodontic treatment in this borderline surgical case.
The diagnosis and orthodontic treatment of Class II Division 1 malocclusions in an adult patient with a brachyfacial skeletal pattern and impinging deepbite can be challenging for the practitioner. The tendency for downward and backward mandibular rotation in response to orthodontic forces of inappropriate magnitude or direction must be minimized. When correcting a Class II deepbite, an important clinical goal is to reduce the amount of overbite. However, when this malocclusion is associated with lip protrusion and significant tooth display, it is also necessary to maximize the anchorage of the posterior teeth during retraction.
Extraoral appliances, such as the J-hook headgear, are effective in both controlling anchorage during anterior tooth retraction and achieving effective intrusion of the incisors, even though a high level of patient cooperation is necessary. In patients with deepbite and excessive tooth display, even in the resting lip position, intrusion of the maxillary incisors is required rather than extrusion of the molars. The J-hook headgear gives excellent control of extrusion of the maxillary posterior teeth.
The amount and direction of force of the J-hook headgear should be considered because it will change the movement of the incisors in both the vertical and horizontal directions. The use of the J-hook headgear in the appropriate direction (high pull) can provide directional forces that will place the teeth in harmonious relationships with their environment and create stable anchorage. However, the intrusion effect might vary, since it depends on complete patient cooperation.
With the increasing popularity of skeletal anchorage, titanium screws have been used in many clinical situations such as intrusion and en-masse retraction of the anterior teeth without the critical problem of patient compliance. However, traditional effective treatment might be considered for patients who do not want surgical or any other invasive intervention.
Diagnosis and etiology
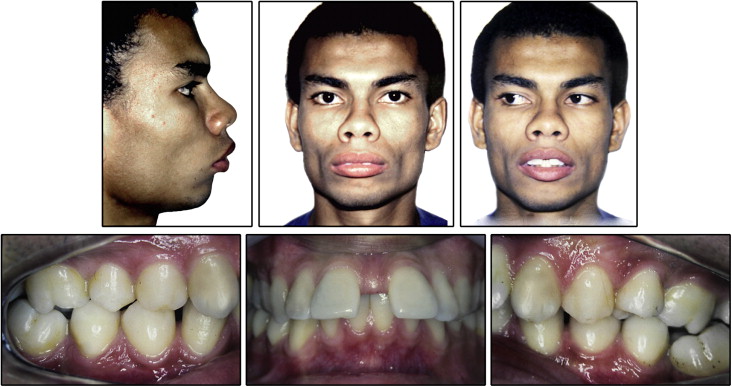
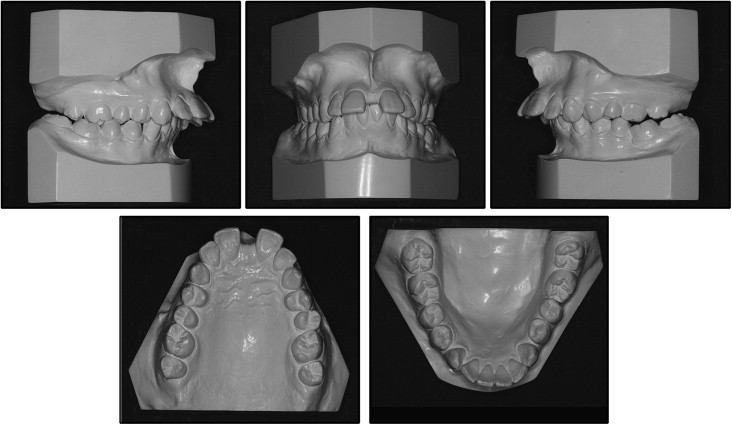
The patient was a 21-year-old man of normal weight and stature with no relevant medical history. His main complaints were lip protrusion and the diastema between the maxillary central incisors. The facial photographs showed a convex facial profile with marked lip protrusion and an everted lower lip, mentalis muscle strain, and a proportionally shorter lower anterior facial height. The temporomandibular joints were clinically normal. He had 2 mm of anterior mandibular dental crowding and a 1-mm diastema distal to each mandibular canine. The mandibular discrepancy was zero. There was a 5-mm diastema between the maxillary central incisors. A space was also evident between the maxillary central and lateral incisors, distally to the maxillary canines. The mandibular dental midline was displaced about 1 mm to the patient’s right. On lip closure, the maxillary central incisors were exposed, as well as with the lips at rest. Both mentalis and maxillary lip strain were observed ( Figs 1 and 2 ).
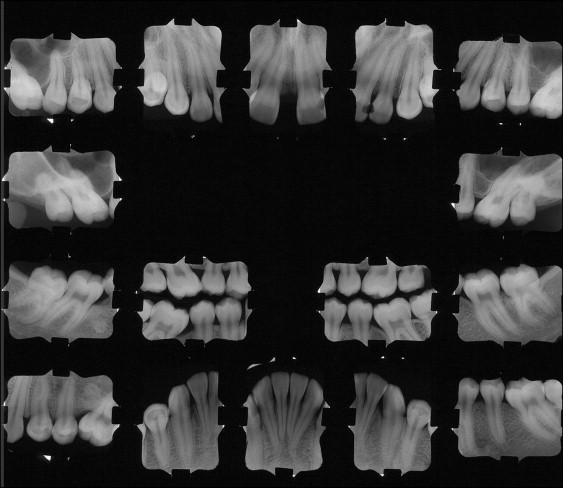
The tooth roots appeared normal radiographically, all amalgam fillings were satisfactory, and both mandibular and maxillary first molars had been extracted because of caries ( Fig 3 ). Oral hygiene was adequate, and the gingival tissues were healthy.
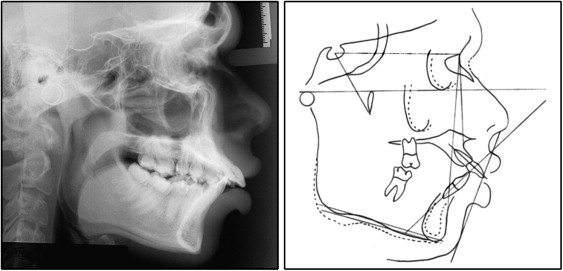
Analysis of the lateral cephalogram ( Fig 4 ) confirmed the skeletal problem. The patient had a brachyfacial skeletal pattern with a low mandibular plane angle (FMA, 17°; SN-GoGN, 22°) and a severe Class II malocclusion (SNA, 95°; SNB, 86°; ANB, 9°; Wits, +6 mm). He had a dentoalveolar Class II Division 1 malocclusion with a 14-mm overjet, an impinging deepbite, and a vestibular posterior crossbite. The maxillary and mandibular central incisors were excessively proclined (1.NA, 41°; 1-NA, 12 mm; 1.NB, 35°; 1-NB, 11.5 mm; IMPA, 113°).
Treatment objectives
The treatment goals were to (1) align and level the teeth in both arches and establish a functional occlusion, (2) maintain the Class II molar relationship of the second molars with a Class I canine relationship, (3) achieve normal overjet and overbite, (4) obtain a balanced facial profile, and (5) improve facial esthetics.
Treatment objectives
The treatment goals were to (1) align and level the teeth in both arches and establish a functional occlusion, (2) maintain the Class II molar relationship of the second molars with a Class I canine relationship, (3) achieve normal overjet and overbite, (4) obtain a balanced facial profile, and (5) improve facial esthetics.
Treatment alternatives
The first alternative was orthognathic surgery. After space closure, 2-jaw surgery including counterclockwise differential impaction of the maxilla and concurrent mandibular advancement surgery would be performed to correct the skeletal discrepancy. Genioplasty would be necessary to advance the chin along the facial midline. However, the patient declined surgical treatment.
The second alternative was orthodontic treatment consisting of the extraction of the 2 maxillary first premolars and directional force technology with microimplant anchorage. The microimplant could provide absolute anchorage, not only to achieve maximum retraction of the maxillary anterior teeth, but also to improve their intrusion. A genioplasty would be necessary to advance the chin to obtain a balanced facial profile. However, the patient declined both the microimplant and the genioplasty surgery but accepted the treatment plan involving the Tweed-Merrifield directional force, with extraction of the 2 maxillary first premolars and the high-pull J-hook headgear as anchorage control during anterior tooth retraction and with an active intrusion force on the incisors.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


