Armamentarium
|
History of the Procedure
Efforts to shorten the mandible to correct mandibular excess and/or mandibular asymmetry have produced a variety of osteotomy designs and surgical instrumentation. Limberg described the oblique subcondylar osteotomy in 1925. Subsequently, Moose and others described intraoral procedures for mandibular reduction. The vertical ramus osteotomy popularized in 1954 by Caldwell and Letterman required an extraoral approach. The sagittal split ramus osteotomy (SSO) described by Trauner and Obwegeser in 1957 was the first intraoral ramus osteotomy that permitted mandibular reduction. In 1968, Winstanley reported the first intraoral vertical ramus osteotomy (IVRO), performed with a dental drill. A significant advance in the IVRO technique was reported by Herbert et al in 1970 with the use of the motorized oscillating saw. The work of Hall et al and Hall and McKenna in the 1970s further popularized the procedure, and Hall’s work in the 1980s helped quantify clinical outcomes and proposed technique refinements to minimize proximal segment “sag.”
History of the Procedure
Efforts to shorten the mandible to correct mandibular excess and/or mandibular asymmetry have produced a variety of osteotomy designs and surgical instrumentation. Limberg described the oblique subcondylar osteotomy in 1925. Subsequently, Moose and others described intraoral procedures for mandibular reduction. The vertical ramus osteotomy popularized in 1954 by Caldwell and Letterman required an extraoral approach. The sagittal split ramus osteotomy (SSO) described by Trauner and Obwegeser in 1957 was the first intraoral ramus osteotomy that permitted mandibular reduction. In 1968, Winstanley reported the first intraoral vertical ramus osteotomy (IVRO), performed with a dental drill. A significant advance in the IVRO technique was reported by Herbert et al in 1970 with the use of the motorized oscillating saw. The work of Hall et al and Hall and McKenna in the 1970s further popularized the procedure, and Hall’s work in the 1980s helped quantify clinical outcomes and proposed technique refinements to minimize proximal segment “sag.”
Indications for the Use of the Procedure
Intraoral vertical ramus osteotomy is indicated for the management of horizontal mandibular excess. Additionally, small distal segment advancement (less than 2 mm) is compatible with IVRO. Intraoral vertical ramus osteotomy is also ideally suited to the management of mandibular asymmetry with planned rotation about one ramus.
For symptomatic temporomandibular disorder, IVRO may be preferred over SSO because the condyle is passively positioned, with little opportunity to place the condyle in an unphysiologic and/or loaded position. Furthermore, experience with modified mandibular condylotomy suggests that IVRO may actually improve joint symptoms.
Limitations and Contraindications
Critics of IVRO initially highlighted unpredictable stability. Hall and McKenna described “condylar sag” caused by stripping of the masseter and medial pterygoid muscles, which led to a 14% incidence of open bite at the time of maxillomandibular fixation (MMF) release. Subsequently, these researchers described a modification of the IVRO technique to preserve medial pterygoid attachment. Intraoral vertical ramus osteotomy should be used cautiously, if at all, when counterclockwise rotation of the distal segment and vertical ramus lengthening are required. Small closing rotations of the mandible may be considered with IVRO, such as with an edge-to-edge incisor relationship. Vertical lengthening of the ramus creates a distracting force on the condylar segment and predisposes to condylar sag and skeletal instability. The same undesirable forces can result with two-jaw surgery in which vertical lengthening of the maxilla is combined with IVRO. As has been noted, small amounts of mandibular advancement may be considered with IVRO. Distal segment advancement is less likely result in condylar sag if simultaneous vertical ramus shortening is planned. Vertical ramus shortening encourages condylar seating (and forward rotation of the proximal segment).
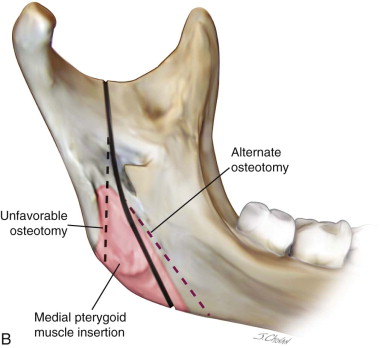
In general, up to 10 mm of mandibular setback is possible with IVRO. Because it is important to preserve as much medial pterygoid muscle attachment as possible, the magnitude of the setback should not exceed the width of the proximal segment medial pterygoid attachment. If the posterior movement of the distal segment exceeds the width of the medial pterygoid attachment, there will be little or no remaining medial pterygoid attachment to the proximal segment. This promotes condylar sags and even condylar subluxation due to unopposed lateral pterygoid activity. Conversely, if insufficient medial pterygoid muscle is stripped from the proximal segment, backward rotation of the segment occurs as the distal segment moves posteriorly, predisposing to postoperative forward relapse.
Internal fixation is technically more difficult with IVRO because of limited visibility and access for fixation instrumentation. However, right-angled drilling and screwdriving instruments have expanded the opportunity for transoral “rigid” internal fixation. In the absence of internal fixation, a period of maxillomandibular fixation is required.
Because IVRO generally is used in the management of horizontal mandibular excess, it is prudent to consider any history of obstructive sleep apnea (OSA) before surgical mandibular reduction. If OSA is suspected, polysomnography should be obtained before mandibular reduction surgery. The potential for mandibular reduction to exacerbate OSA should be considered.
Finally, with two-jaw surgery in which the surgeon prefers to perform mandibular surgery first, SSO generally provides superior internal fixation and osteotomy stability to allow mandible-first surgery.
Technique: Intraoral Vertical Ramus Osteotomy
Step 1:
Incision/Subperiosteal Dissection
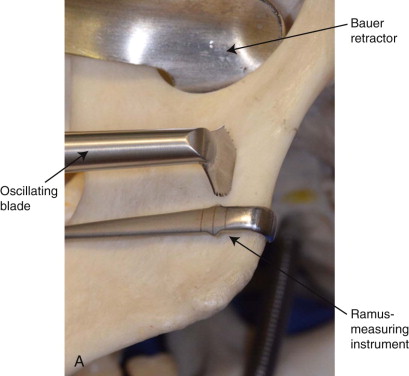
Nasoendotracheal intubation is required. A local anesthetic with epinephrine is infiltrated in the region of the external oblique ridge. In the rare circumstance that preoperative orthodontic preparation is not required, maxillary and mandibular arch bars are applied from first molar to first molar, with ligation of all teeth. Access to the ramus is through a ramus-exposing incision that is made 2 to 3 mm lateral to the mucogingival junction and extends from the level of the occlusal plane to the first molar. Incisions placed more than 2 to 3 mm from the mucogingival junction often create an unacceptable scar band that demarcates a food trap and hygiene nuisance. The lateral periosteum is elevated from the inferior border to the sigmoid notch. The periosteal flap is further released by stripping temporalis tendon from the anterior border of the mandible. The periosteum at the posterior portion of the ramus should not be elevated and the most tenacious attachment of the masseter muscle should be preserved at the inferior border. Use of the Levasseur Merrill retractor is discouraged because this retractor requires posterior border stripping. A Bauer retractor is placed in the sigmoid notch. A second Bauer retractor may be placed at the inferior border, although a single Bauer retractor generally is sufficient for the superior portion of the osteotomy.
Step 2:
Determination of the Osteotomy’s Location
Once exposed, the lateral ramus is carefully inspected. A useful but not entirely reliable landmark is the antilingular prominence, a lateral bony protuberance that approximates the lingula on the medial surface of the ramus. Using the oscillating saw and the 11.5 × 7-mm blade, the surgeon marks the osteotomy location 7 to 8 mm anterior to the posterior border of the mandible at approximately the level of the mandibular foramen. A severely curved Freer elevator is used to estimate the distance from the posterior border to the trial osteotomy. Alternatively, a ramus-measuring instrument and laryngeal mirror or 30-degree endoscope may be used to visualize the planned osteotomy. The trial osteotomy should be just behind the antilingular prominence. If the osteotomy is within or anterior to the antilingular prominence, the mandibular foramen or canal may be violated ( Figure 31-1, A ).

Step 3:
Completion of the Superior Osteotomy
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


