Maxillary and mandibular widening
Mandibular-maxillary deficiency is one of the most common dentofacial deformities. This problem can present in the three dimensions of space: (1) anteroposterior, (2) vertical, and (3) transverse. It also may be combined with other maxillary alterations. In the past, the treatment of this dentofacial problem consisted of either integrated orthodontic-surgical treatment, or orthodontic dental compensations alone. The key to a correct diagnosis of the facial growth alteration is a comprehensive evaluation: the three-dimensional assessment of vertical, anteroposterior, and transverse skeletal and dental positions, and soft tissues. Cephalometric analysis should be performed for every patient to combine the surgical procedures needed to correct the deformities in one surgical intervention. The orthodontist should evaluate the patient for potential initial preoperative orthodontics, root divergence, and prediction for future orthodontic treatment. This new surgical philosophy treats the deformity through calibrated stimulation of the bone: the combination with orthodontics and surgery to correct certain deficiencies of the jaws.
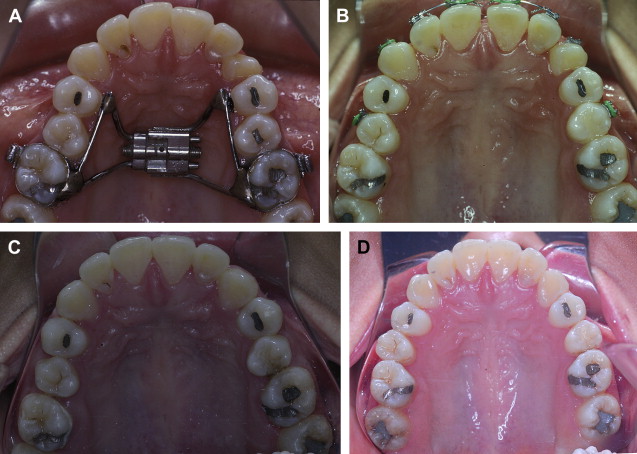
Maxillary widening
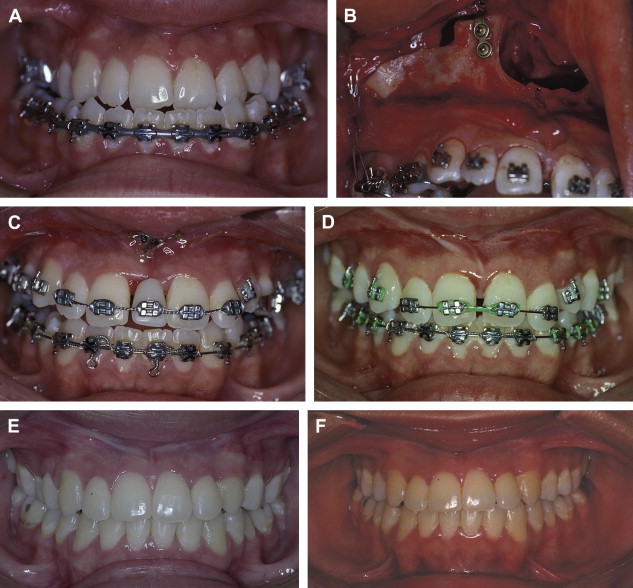
When maxillary widening is needed, a tooth-borne appliance is placed 1 day presurgically, a Le Fort I osteotomy, with a complete downfracture going through the tuberosity instead of through the pterygomaxillary junction. A midline osteotomy is accomplished taking in consideration the nasal structures when the maxilla undergoes a three-dimensional movement, or an asymmetric distraction to correct an occlusal asymmetry ( Figs. 1–10 ). The distraction protocol consists of a 7-day latency period, activation phase at a rate of 1 mm per day until desired movement is obtained, an immediate placement of an acrylic tooth added to the orthodontic arch at the distraction site, and switching the dental-borne appliance by a transpalatal bar for a 5- to 7-month consolidation period.

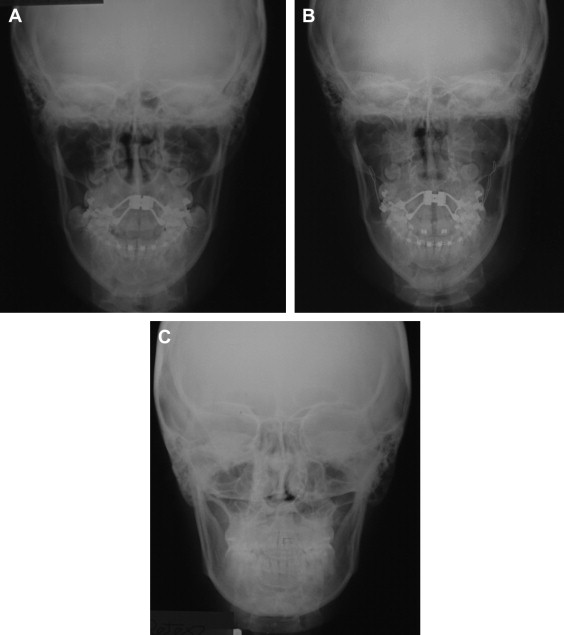
A three-dimensional treatment can be planned for the maxilla in one single stage. The age of treatment is based on three major considerations: (1) the canine eruption level, (2) the anatomic situation of the infraorbital nerve, and (3) the nasolachrymal duct. Patients with bidimensional or three-dimensional maxillary deficiencies can be treated by intraoral distraction osteogenesis to lengthen, widen, or augment vertically the maxillomalar complex at different osteotomy levels according to the individual clinical situation. Complete radiographs and photographs are obtained presurgery, immediately postsurgery, 3 months later, at the appliance removal stage, and 6 months after braces are removed. Dental models in an articulator should be taken before the surgery and after removal of braces.
These patients should undergo a combined surgical-orthodontics treatment ideally to correct the tridimensional problems. In those requiring a high Le Fort I, a conventional incision and osteotomy is accomplished, the maxilla is freely moved, and distractors are placed bilaterally anchored to the base of the zygoma and fixed to the maxilla with the adequate vector based on the three-dimensional planning. A modified Le Fort III has an additional transconjunctival approach: the osteotomy divides the malar process, runs medially above the infraorbital nerve, the orbital floor is sectioned behind the infraorbital rim continuing underneath and obliquely anterior to avoid the nasolachrymal duct reaching the piriform rim, and posteriorly extended to the pterygo-maxillary suture. Finally, two wide-curved osteotomes are placed behind the maxillary tuberosities to displace the malar-maxillary complex. Once it is completely freed, the distractors are fixed, the posterior bar is screwed to the zygoma with 2.0 screws, and the anterior bar is fixed to the maxilla above the teeth.
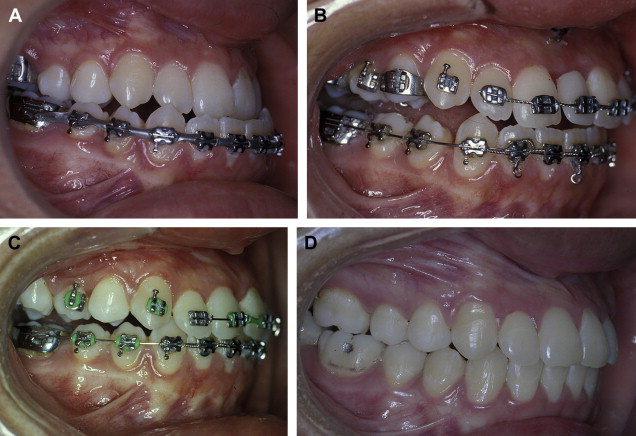
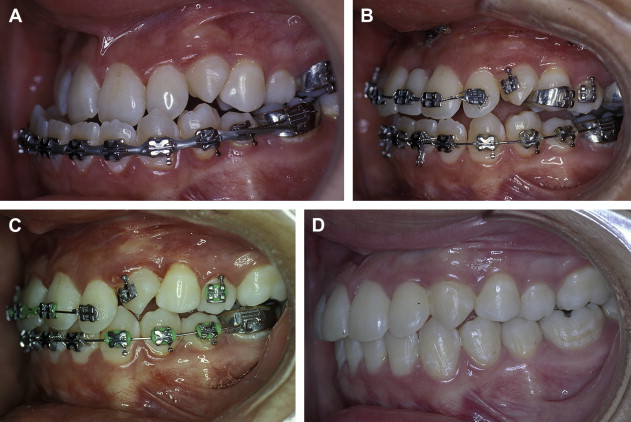
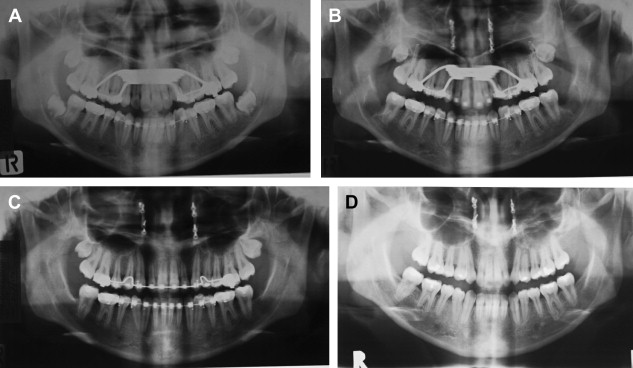
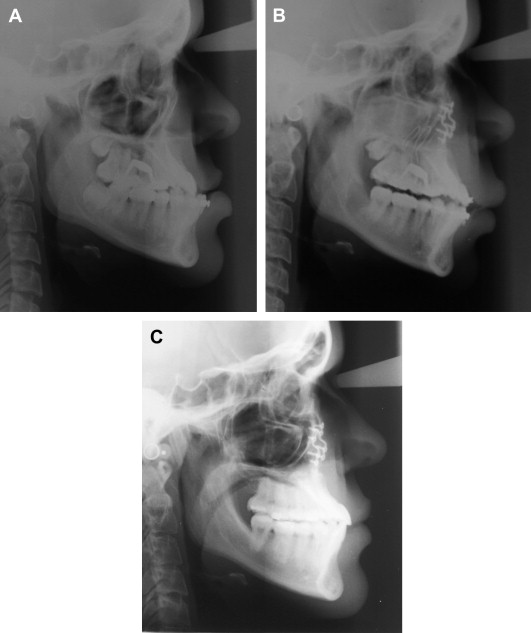
Mandibular widening
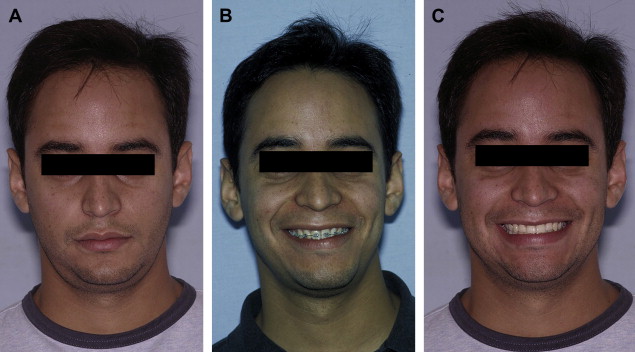
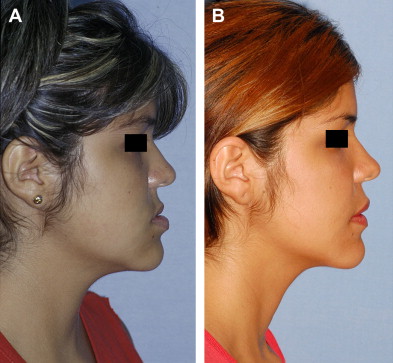
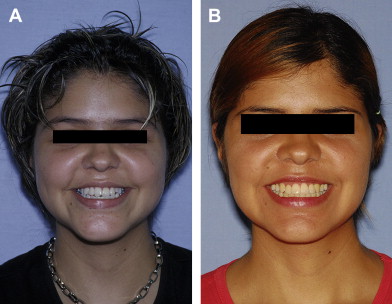
The severe crowding in a patient is usually part of a micrognathia, which includes a deficiency in growth in all three planes with skeletal and dental problems. In the past, dental crowding was treated by compensatory orthodontics and dental extraction, obtaining unstable results or extremely narrow dental arches with tunnel smiles ( Figs. 11–22 ). Because the functional matrix dictates the development of both maxilla and mandible, it is predictable that most of cases with skeletal class II and narrow arch present a problem with the maxilla. It is imperative to make a three-dimensional analysis to provide correct three-dimensional treatment.