Vertical dentoalveolar discrepancies are a common problem in orthodontic patients but are often difficult to treat with traditional mechanics. This case report illustrates the successful treatment of overerupted mandibular incisors via the indirect use of miniscrew anchorage. A woman (age, 22 years 9 months) had chief complaints of maxillary incisor protrusion and crooked teeth. An excessive curve of Spee caused by elongation of the mandibular incisors was also found. The patient was diagnosed with a severe Class II Division 1 malocclusion and a deep overbite. After extraction of the mandibular first premolars and the subsequent leveling phase, the elongated incisors were intruded with a novel method, which involved the combined use of sectional archwires and miniscrews placed in the premolar areas. After the procedure, the mandibular incisors had been intruded by 6.5 mm with no undesirable side effects. The total active treatment period was 42 months. The resultant occlusion and satisfactory facial profile were maintained after 30 months of retention. Our novel intrusion approach shows potential for correcting a deep overbite.
A deep overbite is a common malocclusion and is typically corrected by intrusion of the anterior teeth or extrusion of the posterior teeth. Several mechanical methods involving multibracket treatment have been proposed for incisor intrusion. Molar extrusion and subsequent posterior rotation of the mandible should be observed, whether continuous or sectional archwires are used for the intrusion, since they obtain their anchorage from the posterior teeth. Clockwise rotation of the mandible can also improve a deep overbite; however, it can worsen the facial profile of patients with a skeletal Class II jaw relationship.
Recently, implant-anchored orthodontics have led to the development of new orthodontic treatment strategies. These implants can provide stationary anchorage for various tooth movements and even make it possible to move a tooth in more than 1 direction; this was impossible with traditional orthodontic methods. Miniscrew anchorage is especially useful for tooth intrusion, because it can apply a low, continuous force of a set magnitude without causing reciprocal movements of other teeth.
This article describes the successful treatment of an adult patient with a Class II Division 1 malocclusion, a deep overbite, and an excessive mandibular curve of Spee by using miniscrew anchorage and segmented wires.
Diagnosis and etiology
A woman, 22 years 9 months old, came to the outpatient clinic of Okayama University Hospital in Japan. Her chief complaints were protruding maxillary incisors and crooked teeth ( Figs 1-3 ). She had a convex profile and an acute nasolabial angle and suffered from circumoral musculature strain on lip closure. An excessive overjet of 8.3 mm and a deep overbite of 5.1 mm were also observed. In addition, an excessive curve of Spee of 5.0 mm was found in the mandibular arch, and the left first premolars had a scissors-bite ( Fig 3 ). Both dental arches were constricted, especially the mandibular arch. Severe crowding was observed in the mandibular incisors ( Figs 3 and 4 ). The maxillary dental midline almost coincided with the facial midline and the mandibular dental midline. The interincisal distance on maximal opening without pain was 48 mm.

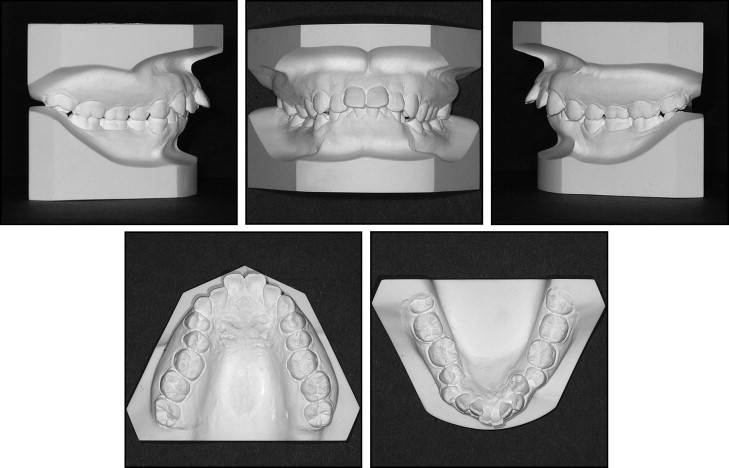
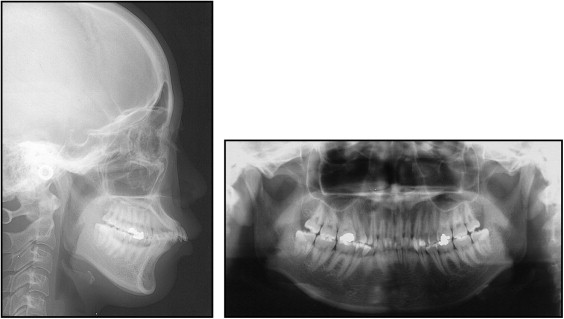
In a comparison with Japanese norms, her cephalometric analysis showed a skeletal Class II jaw relationship (ANB, 6.5°), an average mandibular plane angle (Mp-FH, 28.5°), a normal gonial angle (125°), and excessive anterior lower facial height (Me/PP, 75.0 mm) ( Table ). The maxillary and mandibular incisors were labially inclined (U1-FH, 130.4°; L1-Mp, 105.5°). The mandibular incisors were significantly extruded (L1/Mp, 53 mm), and she had severe Class II molar relationships on both sides.
| Variable | Japanese norms for women | SD | Pretreatment | Postintrusion |
|---|---|---|---|---|
| Angular (°) | ||||
| ANB | 2.8 | 2.44 | 6.5 | 6.5 |
| SNA | 80.8 | 3.61 | 83.0 | 83.0 |
| SNB | 77.9 | 4.54 | 76.5 | 76.5 |
| Mp-FH | 30.5 | 3.60 | 28.5 | 28.5 |
| U1-FH | 112.3 | 8.26 | 130.5 | 105.5 |
| U1-SN | 105.9 | 8.79 | 122.5 | 97.5 |
| L1-Mp | 93.4 | 6.77 | 105.5 | 107.0 |
| Interincisal angle | 123.6 | 10.64 | 95.5 | 119.5 |
| Occlusal plane | 16.9 | 4.40 | 12.0 | 19.0 |
| Linear (mm) | ||||
| S-N | 67.9 | 3.65 | 69.0 | 69.0 |
| N-Me | 125.8 | 5.04 | 131.0 | 131.0 |
| Me/PP | 68.6 | 3.71 | 75.0 | 75.0 |
| Go-Me | 71.4 | 4.14 | 72.0 | 72.0 |
| Ar-Me | 106.6 | 5.74 | 112.0 | 112.0 |
| Ar-Go | 47.3 | 3.33 | 52.0 | 52.0 |
| Overjet | 3.1 | 1.07 | 8.3 | 3.5 |
| Overbite | 3.3 | 1.89 | 5.1 | 3.1 |
| U1/PP | 31.0 | 2.34 | 33.0 | 35.5 |
| U6/PP | 24.6 | 2.00 | 28.5 | 28.5 |
| L1/Mp | 44.2 | 2.68 | 53.0 | 48.0 |
| L6/Mp | 32.9 | 2.50 | 37.0 | 37.5 |
Treatment objectives
The patient was diagnosed with an Angle Class II malocclusion, a skeletal Class II jaw-base relationship, and severe crowding with a deep overbite caused by overerupted mandibular incisors. The treatment objectives were to create a more ideal overbite and overjet relationship, correct her excessive curve of Spee, reduce the anteroposterior skeletal discrepancy, improve her facial profile, and obtain Class I canine and molar relationships. We planned to use miniscrews for absolute anchorage, because of the complexity of the patient’s problems: ie, a Class II patient with a deep overbite and an excessive curve of Spee.
Treatment objectives
The patient was diagnosed with an Angle Class II malocclusion, a skeletal Class II jaw-base relationship, and severe crowding with a deep overbite caused by overerupted mandibular incisors. The treatment objectives were to create a more ideal overbite and overjet relationship, correct her excessive curve of Spee, reduce the anteroposterior skeletal discrepancy, improve her facial profile, and obtain Class I canine and molar relationships. We planned to use miniscrews for absolute anchorage, because of the complexity of the patient’s problems: ie, a Class II patient with a deep overbite and an excessive curve of Spee.
Treatment alternatives
One therapeutic method proposed for the treatment of a Class II malocclusion and overerupted mandibular incisors with a deep overbite involves a combination of comprehensive orthodontic treatment and orthognathic surgery. However, this approach was considered to be too aggressive and invasive for this patient. In addition, she wished to avoid orthognathic surgery.
Another alternative was nonminiscrew anchorage treatment. However, anchorage control in patients suffering from severe skeletal Class II malocclusion is a difficult problem. Moreover, for this patient, this method would have led to molar extrusion, which would have worsened her skeletal Class II jaw relationships and excessive overjet. In addition, absolute intrusion of the overerupted incisors would have been impossible without absolute anchorage. Thus, absolute anchorage was considered to be essential to achieve the treatment objectives. Miniplates were considered as alternatives, but they require a more invasive procedure than does miniscrew anchorage.
Treatment progress
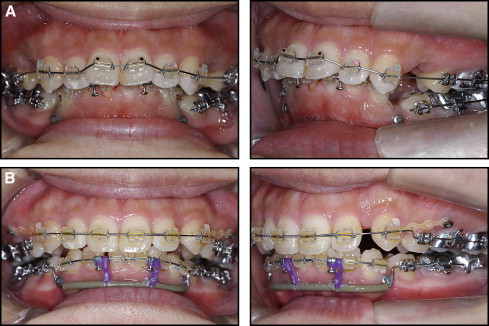
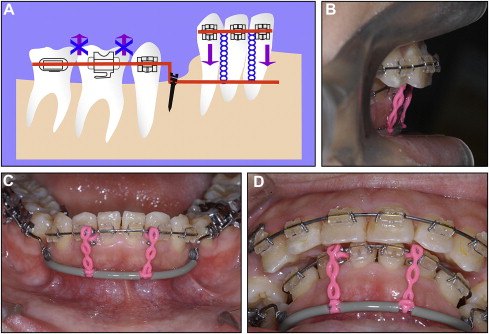
Initially, the narrow maxillary and mandibular dental arches were treated with a quad-helix appliance and an expanded lingual arch appliance for 4 months, respectively. After extraction of the maxillary and mandibular first premolars, an 0.018-in preadjusted edgewise appliance was placed in the mandibular arch. Initial alignment was achieved with 0.012-in nickel-titanium sectional archwires. Miniscrews (length, 9 mm; diameter, 1.5 mm; Martin, Tuttlingen, Germany) were placed into the buccal alveolar bone at the mandibular premolar extraction sites to achieve en-masse intrusion of the mandibular anterior teeth. Two months after leveling and alignment of the mandibular arch, stainless steel wires were installed to coordinate the arch forms. Simultaneously, an 0.018-in preadjusted edgewise appliance was placed into the maxillary arch. Initial alignment was achieved with a 0.016-in nickel-titanium archwire. Miniscrews were also implanted between the roots of the maxillary second premolar and first molar to reinforce the posterior anchorage during anterior tooth retraction. After screw placement, a 0.016- × 0.022-in utility archwire (Blue Elgiloy; Rocky Mountain Morita, Tokyo, Japan) was installed and ligated to the mandibular miniscrews before en-masse intrusion of the mandibular anterior teeth. Elastic chains were tied between the utility archwire and the anterior segment of sectional archwire ( Fig 4 ). In this system, we applied a continuous intrusive force of 50 g.
Eight months after the intrusion of the mandibular anterior teeth ( Fig 5 ), the miniscrews were removed, and a 0.016 × 0.022-in continuous beta-titanium archwire with a reverse curve of Spee was placed in the mandibular arch. After leveling and alignment of the mandibular arch, 0.017 × 0.025-in stainless steel archwires were installed for anterior tooth retraction. Then, the stainless steel wires were positioned to coordinate the 2 arch forms. In anticipation of some relapse, the patient’s overjet and overbite were overcorrected. The total active treatment period was 42 months. After removing the appliances, the maxillary and mandibular teeth were stabilized by using a 6-unit lingual bonded retainer and a Begg-type retainer.