Introduction
The purpose of this study was to determine the dimensional changes that occur in the alveolar ridge of patients upon distalization of the mandibular first premolars into the place of congenitally missing mandibular second premolars. The amount of bone formation that accompanied orthodontic treatment and the long-term stability of the new bone were assessed.
Methods
Fifty-five patients were included in the study, representing 71 congenitally missing mandibular second premolars. The dimensional changes were evaluated by comparing the dental stone casts and panoramic radiographs taken at treatment initiation (T1) and end (T2) and at follow-ups of 2 years (T3A) and 5 years (T3B).
Results
During the treatment period (T1-T2), the alveolar ridge width increased by an average of 28.5%, and the height increased by an average of 1.1 mm. During the retention periods (T2-T3A, T2-T3B), the alveolar ridge decreased by an average of 4.2%, but the height decreased only slightly (by an average of 0.07 mm).
Conclusions
Orthodontic tooth movement created a significant amount of new bone that was stable in both the horizontal and vertical directions.
Studies on the stability and esthetic aspects of implantation-based treatments have shown that these 2 features strongly depend on the quality and quantity of bone mass available for implant placement. In patients whose ridge dimensions are insufficient for placement, bone grafting has proved useful; however, recent studies have indicated that orthodontic tooth movement might be a useful alternative to a bone graft. The changes that occur in the supporting tissues after orthodontic tooth movement are well known and documented: the force generates bone resorption on the pressure side and bone apposition on the tension side. The formation of the bone can be achieved in both the vertical and horizontal planes.
In the vertical direction, the orthodontic extrusion (extraction) can improve the local hard-tissue and soft-tissue profiles of implant recipient sites. The movement does not create a new attachment, but relocates the existing attachment in a coronal direction. The bone follows the tooth, whereas soft tissues follow the extruded tooth for about 80% of the distance. The procedure was introduced in 1993 to manipulate nonrestorable “hopeless” teeth to modify their local defect environment before extraction.
In the horizontal plane, as a tooth is moved orthodontically through the alveolus into an edentulous space, remodeled bone forms behind the root, which in turn promotes creation of new bone. Bodily tooth movement can be an interesting option to bone grafting in situations where dimensional alterations of the alveolar ridge often occur, such as (1) agenesis of a maxillary lateral incisor (distal movement of a canine that was allowed to erupt mesially into the lateral incisor space), (2) agenesis of a maxillary second premolar or an edentulous maxillary molar area (distal movement of a premolar through the maxillary sinus), (3) agenesis of a mandibular second premolar (distal movement of a mandibular first premolar), or (4) an edentulous mandibular molar region (distal movement of a mandibular second premolar).
Several authors have assessed the amount and the stability of this newly created bone; most of these studies have focused on patients with agenesis of maxillary lateral incisors who were treated with distalization of the canine. The second most common form of tooth agenesis involves the mandibular second premolars, but the literature offers only a few case series dealing with this problem.
Thus, this retrospective study was designed to investigate the changes in bone mass that occur in the vertical and horizontal dimensions during orthodontic treatment (distalization of the mandibular first premolar to the place of the missing mandibular second premolar), to determine the changes in the alveolar ridge dimensions after a period of retention (2 or 5 years), and to assess whether these long-term changes differed among patients with inserted endosseous dental implants and patients without implants.
Material and methods
Fifty-five patients with a total of 71 sites with missing mandibular second premolars were enrolled in the study. The patients were recruited from 5 private orthodontic practices in Břeclav, Kroměříž, Náchod, Praha, and Třinec and the Department of Orthodontics, Medical Faculty, University of Palacký, Olomouc, Czech Republic.
The following selection criteria were used: (1) the patient must have at least 1 mandibular second premolar missing and had undergone complete orthodontic treatment with fixed appliances; (2) the treatment must have involved distalization of the mandibular first premolar; and (3) the patient’s records must have included good-quality panoramic radiographs and dental stone casts taken at orthodontic treatment initiation (T1) and end (T2) and at the retention period (T3), either 2 years after treatment (T3A) or 5 years after treatment (T3B).
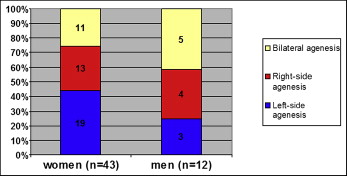
The study population was predominantly female (n = 43). There was bilateral absence of the mandibular second premolars in 16 patients; the remaining 39 patients had unilateral absence, with left-side absence in 22 and right-side absence in 17 ( Fig 1 ). The ages of the total subjects ranged from 11 to 52 years; they were 11.6 to 47.2 years (mean, 22.7) at T1, 14.1 to 50.5 years (mean, 25.4) at T2, 17.4 to 52.7 years (mean, 34.2) at T3A, and 18.5 to 48.8 years (mean, 25.7) at T3B.
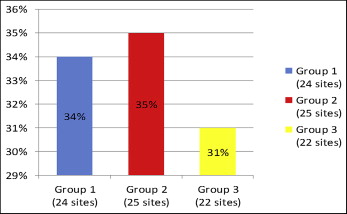
For analysis, the study population was divided into 3 groups according to the newly formed bone at the alveolar ridge: group 1, free of implant at retention (20 patients with 24 sites that were missing mandibular second premolars); group 2, endosseous dental implants at the retention period (20 patients with 25 edentulous sites); and group 3, no data for the retention period were available; only the dimensional changes that occurred during orthodontic treatment (T1-T2) were assessed (15 patients with 22 edentulous sites) ( Fig 2 ).
The dental stone cast analysis and the radiographic analysis were based on the studies of Ostler and Kokich and Nováčková et al.
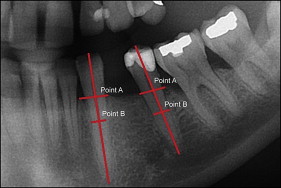
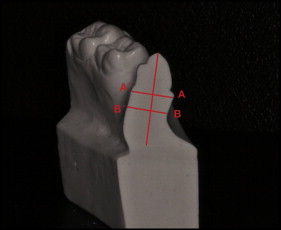
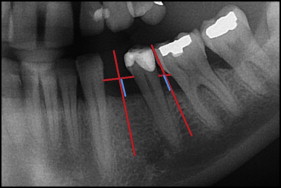
The points measured on the dental casts were first determined with panoramic radiographs. At T1, the distance was measured between the tip of the vestibular cusp of the first premolar and the first premolar alveolar ridge (Point A) in the long axis of the tooth. Point B was then set at 5 mm apically from Point A. The same measurement was made for the mandibular first molar; specifically, the distance was measured between the tip of its mesio-vestibular cusp and the molar alveolar ridge (Point A) in the long axis of the tooth, with Point B set at 5 mm apically. At T2 and T3, the same measurements were taken for the canine and the distalized first premolar ( Fig 3 ).
In the dental stone cast analysis, the width of the alveolar ridge was measured with a digital caliper at Point A (level of the bony alveolar ridge) and at Point B (5 mm apically to the alveolar ridge). The edentulous ridge area was the study focus; at T1, the measurements were taken at the place of the missing mandibular second premolar between the first molar and the first premolar and then, at T2 and T3, at the newly created edentulous space between the canine and the distalized mandibular first premolar. In 15 patients with unilateral agenesis, the opposite side was measured for the control data; this measurement assessed the thickness of the alveolar ridge at the sites of the first and second premolars.
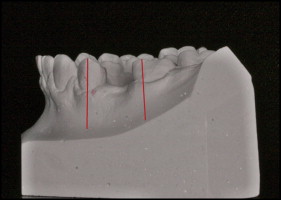
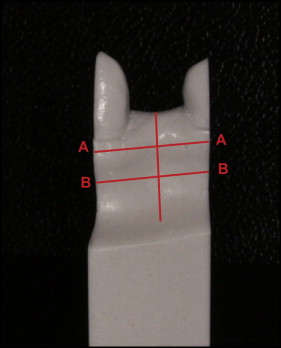
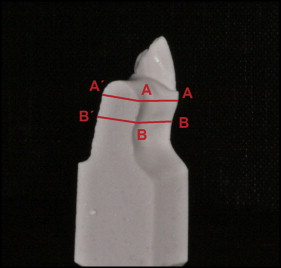
The dental stone casts taken at T1 were cut vertically on the long axes in the middle of the vestibular cusps of the first premolars and in the middle of the mesio-vestibular cusps of the first molars ( Fig 4 ). For the sectioned dental casts, the long axes of the first premolars and first molars were lowered from the vestibular (ie, mesio-vestibular) cusp, and Points A and B were traced ( Fig 5 ). A perpendicular line was made from Point A for both the vestibular and lingual sides. The same process was followed for Point B. In addition, a line was made from the middle of the site of the missing second premolar perpendicular to the occlusal plane, and then Points A and B that were set for the first premolar and the first molar were connected from both the vestibular and lingual sides ( Fig 6 ). At the intersections, Points A and B from the vestibular and lingual sides for the edentulous ridge were determined. The sectioned dental cast was then further cut vertically, following the line established in the middle of the edentulous space. The connection of the vestibular and the lingual Points A and B represented the thickness of the edentulous alveolar ridge at these 2 levels ( Fig 7 ).
For the dental stone casts taken at T2 and T3, the same method was used, but with measurements for the canine and the distalized first premolar. Ultimately, the distances that were measured during orthodontic treatment (T1-T2) were compared with those after treatment (T2-T3A and T2-T3B).
The height of the alveolar ridge at the site of the missing second premolar was measured at T1, T2, and T3. A line was made between the cementoenamel junctions of the adjacent teeth at T1 between the first premolar and the first molar, and at T2 and T3 between the canine and the distalized first premolar. Then, from the middle of this line, a perpendicular to the occlusal plane was extended to the alveolar ridge and measured ( Fig 8 ). The alveolar ridge level that was measured between the first premolar and the first molar before orthodontic treatment was compared with that after distalization of the first premolar.
Statistical analysis
All statistical analyses were performed with the Statistical Package for the Social Sciences (version 15; SPSS, Chicago, Ill). The differences in thickness of the alveolar ridge at Points A and B at T1, T2, and T3 were evaluated by pairwise comparisons with the Student t test. Statistical significance was established at P <0.05. Since there were multiple tests, the Bonferroni correction was applied, so that the comparison of 5 measurements was adjusted as α = 0.05/5 = 0.01 (ie, threshold of significance: P <0.01).
The measurement error was established by randomly selecting 10 patients for repeated assessments of their dental stone casts and radiographic measurements by the same investigator (P.E.) at least 3 weeks after the original assessments. Statistical analysis of the differences between the first and second measurements was performed. To calculate the measurement errors, Dahlberg’s formula was used. The errors of the width of the alveolar ridge were 0.29 mm at the site of the missing second premolar and 0.13 mm at the site of the first premolar, and the error of the height of the alveolar ridge was 0.27 mm; all values were considered acceptable.
Results
In the edentulous site at Point A, the mean labiolingual width of the new alveolar ridge was 28.5% (1.63 mm) larger after the distalization of the first premolar (T1-T2). The minimum widths were 3.5 mm at T1 and 7.9 mm at T2. The maximum widths were 5.5 mm at T1 and 9.8 mm at T2. At Point B, the alveolar ridge widened by 5.3% (0.47 mm) from T1 to T2. The minimum widths were 5.7 mm at T1 and 6.3 mm at T2. The maximum widths were 11.6 mm at T1 and 13.2 mm at T2 ( Tables I and II ).
| Group 1 | Group 2 | Group 3 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean (mm) | SD (mm) | Max (mm) | Min (mm) | n | Mean (mm) | SD (mm) | Max (mm) | Min (mm) | n | Mean (mm) | SD (mm) | Max (mm) | Min (mm) | |
| Width of edentulous ridge at Point A | |||||||||||||||
| T1 | 24 | 5.61 | 0.93 | 7.4 | 3.5 | 25 | 5.4 | 1.01 | 7.9 | 3.9 | 22 | 6.12 | 0.71 | 7.7 | 5.1 |
| T2 | 24 | 6.80 | 0.79 | 8.5 | 5.5 | 25 | 7.53 | 0.66 | 9.8 | 6.6 | 22 | 7.70 | 0.89 | 10.0 | 6.0 |
| T3A | 14 | 6.66 | 0.85 | 8.2 | 5.3 | 17 | 7.38 | 0.81 | 9.8 | 6.3 | |||||
| T3B | 10 | 6.18 | 0.95 | 7.9 | 4.6 | 8 | 7.36 | 0.5 | 8.0 | 6.4 | |||||
| Width of edentulous ridge at Point B | |||||||||||||||
| T1 | 24 | 8.53 | 1.36 | 10.4 | 5.7 | 25 | 10.29 | 1.10 | 14.0 | 9.0 | 22 | 9.36 | 1.13 | 11.1 | 7.1 |
| T2 | 24 | 8.79 | 1.24 | 11.3 | 6.3 | 25 | 9.97 | 1.02 | 13.5 | 8.7 | 22 | 9.86 | 0.87 | 11.6 | 7.9 |
| T3A | 14 | 8.44 | 1.19 | 10.6 | 6.3 | 17 | 9.73 | 1.24 | 13.8 | 8.1 | |||||
| T3B | 10 | 8.36 | 1.32 | 9.8 | 5.6 | 8 | 9.71 | 0.78 | 10.8 | 8.6 | |||||
| n | Mean (mm) | Median (mm) | SD | Min (mm) | Max (mm) | Change T1-T2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| % | Mean (mm) | SD | P | |||||||
| Point A | ||||||||||
| T1 | 71 | 5.71 | 5.80 | 0.94 | 3.50 | 7.90 | +28.5% | +1.63 | 1.14 | <0.0001 ∗ |
| T2 | 71 | 7.34 | 7.30 | 0.87 | 5.50 | 9.80 | ||||
| Point B | ||||||||||
| T1 | 71 | 8.88 | 9.00 | 1.27 | 5.70 | 11.60 | +5.3% | +0.47 | 0.83 | <0.0001 ∗ |
| T2 | 71 | 9.34 | 9.30 | 1.13 | 6.30 | 13.20 | ||||
For the retention period at 2 years after the treatment (T2-T3A), the alveolar ridge at Point A was reduced by 2.5% (0.18 mm) and by 2.7% (0.25 mm) at Point B ( Table III ). The overall change from T1 to T3A at Point A was 1.45 mm (1.63 − 0.18; SD, 0.28; P <0.0001), with the width of the alveolar ridge widened by 26%. The overall change at Point B was 0.22 mm (0.47 4− 0.25; SD, 0.43; P <0.0001), with the width increased by 2.6%.
| n | Mean (mm) | SD | Change T2-T3A | ||||
|---|---|---|---|---|---|---|---|
| % | Mean (mm) | SD | P | ||||
| Group 1 + group 2 | |||||||
| Point A | |||||||
| T2 | 31 | 7.24 | 0.84 | −2.5% | −0.18 | 0.24 | <0.0001 ∗ |
| T3A | 31 | 7.06 | 0.89 | ||||
| Point B | |||||||
| T2 | 31 | 9.09 | 1.21 | −2.7% | −0.25 | 0.31 | 0.001 ∗ |
| T3A | 31 | 8.84 | 1.16 | ||||
| Group 1 (without implant) | |||||||
| Point A | |||||||
| T2 | 14 | 6.93 | 0.87 | −3.8% | −0.26 | 0.16 | <0.0001 ∗ |
| T3A | 14 | 6.66 | 0.85 | ||||
| Point B | |||||||
| T2 | 14 | 8.72 | 1.20 | −3.2% | −0.28 | 0.36 | 0.013 |
| T3A | 14 | 8.45 | 1.19 | ||||
| Group 2 (with implant) | |||||||
| Point A | |||||||
| T2 | 17 | 7.50 | 0.75 | −1.6% | −0.12 | 0.27 | 0.091 |
| T3A | 17 | 7.38 | 0.81 | ||||
| Point B | |||||||
| T2 | 17 | 9.39 | 1.16 | −2.3% | −0.22 | 0.41 | 0.041 |
| T3A | 17 | 9.17 | 1.06 | ||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


