Treatment of impacted dilacerated incisors is challenging for clinicians because of the prominent position of the teeth and the abnormality of their roots. We report on 2 patients who had horizontally upward impacted and severely dilacerated maxillary central incisors. The first patient’s root perforated the labial plate without significant resorption, and the second patient’s root was resorbed. Both patients were treated by a surgical-orthodontic approach, and the crowns of the impacted teeth were brought into the arches by closed forced eruption. Therefore, if impacted teeth have dilacerated roots, patients should be told of the possibility of root resorption.
Highlights
- •
Impacted maxillary central incisor with severely dilacerated root can be forcibly erupted.
- •
In patient 1, the root perforated the labial plate without significant resorption.
- •
In patient 2, the root was resorbed by touching the labial plate during torque control.
- •
Impacted teeth with dilacerated roots might require endodontic therapy.
- •
Long-term follow up might be necessary depending on the appearance of root resorption.
By virtue of their location, impacted maxillary central incisors in children pose a disturbing esthetic dilemma for parents. Because they are located up front, they are quite obvious when impacted. Space for the incisor tends to close during the delay of eruption, shifting the dental midline. Although impaction occurs less frequently in the maxillary incisors than in the maxillary canines, it is more significant in the early mixed dentition in terms of both esthetics and occlusion.
Many factors can affect the prognosis of impacted teeth, such as the position and direction of the tooth, age of the patient, dilaceration, and so on. Of these factors, dilaceration is a primary obstacle to successful alignment. Impacted incisors show various angulations in the crown or root; the most complicated situation is dilaceration with the crown in an inverted orientation. Depending on the direction and angulation of the dilaceration, ankylosis, external root resorption, and root exposure can occur after orthodontic traction.
Maxillary central incisor eruption failure can be the result of trauma-induced dilacerations. Although the cause of root dilaceration is still unclear, studies have documented several potential causes. Smith and Winter reported that traumatic injury to the deciduous incisors can lead to dilacerations of the permanent incisors, and Kolokithas and Kawakasis found that trauma can cause a change in the axial inclination of an unerupted deciduous incisor.
When trauma occurs before the permanent teeth have erupted, the root-forming cells of the unerupted permanent tooth germ can be damaged, thus impairing the growth of the root and also changing the orientation of the tooth in the alveolar process. The outcome is a dilacerated tooth, which usually requires assistance to erupt. Other trauma-related clinical problems such as ankylosis and invasive cervical root resorption can cause unerupted teeth.
Surgical exposure followed by orthodontic traction is the solution most widely adopted to save impacted dilacerated incisors, but dilacerated roots make the traction complicated and can lead to the need for multiple surgeries not only to enhance effective traction but also to improve gingival esthetics. The prognosis of the treatment depends on the degree of dilaceration, the position of the tooth, and the root formation of the tooth. A dilacerated tooth with an obtuse inclination angle, a closer position to the alveolar crest, and incomplete root formation has a better prognosis for orthodontic traction.
We present 2 young girls with impacted maxillary central incisors and severely dilacerated roots.
Case reports
Patient 1
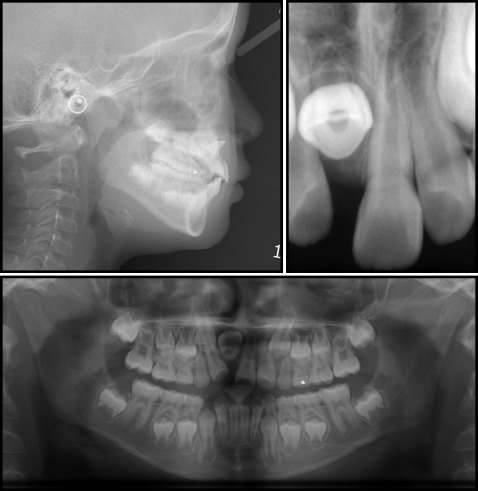
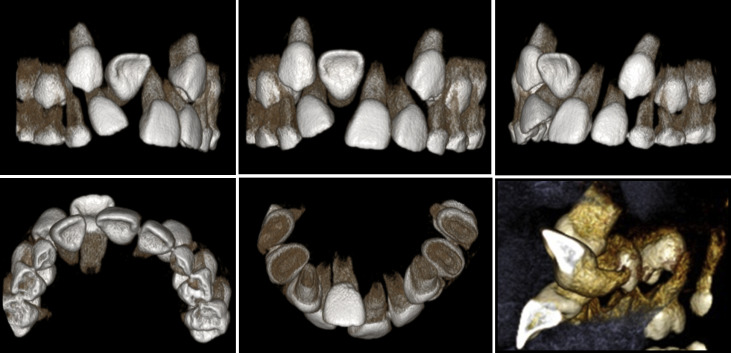
Patient 1 was a 7-year-old girl with the chief complaint of an impacted maxillary right central incisor. There was nothing relevant in her medical or dental history. She had an impacted maxillary right central incisor, which, along with the left central incisor, was tilted into the open space, and the dental midline of her maxillary arch was deviated by 2.5 mm to the right ( Fig 1 ). Radiographs confirmed that the maxillary right central incisor was impacted with dilaceration on the root ( Fig 2 ). The cone-beam computed tomography (CBCT) images taken for further evaluation showed that the crown of the maxillary right central incisor was just below the nasal floor in the premaxilla, with the palatal surface facing forward. Compared with the maxillary left central incisor, the root of the impacted incisor was short, and the apical third was dilacerated upward ( Fig 3 ).

Several treatment options were considered. The first was to extract the impacted maxillary right central incisor to gain space for an implant and fixed prosthetics after the patient was fully grown. The second was to extract the impacted maxillary right central incisor and close the space using fixed orthodontic appliances. After space closure, the right lateral incisor and canine could be treated with prosthetic restorations. The third was to gain space for the maxillary right central incisor with an orthodontic appliance while forcing its eruption. Because the parents wished to bring the impacted tooth down rather than extracting it, the third treatment option was chosen. The patient and her parents were informed of the possibility of root resorption and perforation of the labial bone and therefore the subsequent need for canal treatment and apicoectomy.
Orthodontic treatment using a fixed appliance was initiated to gain space for the maxillary right central incisor. After initial alignment with a 0.014-in nickel-titanium archwire, an 0.018-in stainless steel wire and a nickel-titanium open-coil spring were applied between the maxillary right deciduous canine and left central incisor. After 3 weeks, the impacted maxillary right central incisor was exposed under local anesthesia, and a button was bonded on the lingual surface for forced eruption. The traction of the maxillary right central incisor was started on the day of surgery with elastic thread that was replaced every 4 weeks. After 8 months of treatment, the maxillary right central incisor emerged into the oral cavity, making it possible to bond a bracket on the labial surface of the tooth. Forced eruption continued for 3 more months, but since the deciduous teeth were exfoliating, we decided to remove the appliance and wait ( Fig 4 ).



