External (Open) Approach
A myriad of surgical approaches have been described to expose the nasal skeleton. Two common basic surgical approaches are described here, each with its own set of incisions and modifications. The closed or endonasal approach places all incisions within the nasal cavity so that they are inconspicuous. The open or external approach combines internal and external incisions. This section is divided into two chapters on the basis of these two approaches. Surgical anatomy is discussed in Chapter 13.
|
The nasal skeleton is exposed during many procedures, such as rhinoplasty, septoplasty, fracture management, and reconstructive surgery. It is the only approach described in this book that involves a skeleton that is made of both bone and cartilage.
SURGICAL ANATOMY
The nose has the form of a triangular pyramid, with its summit corresponding to the root of the nose and a base into which the two nostrils open.
External Nasal Bony Framework
The bony framework of the nose consists of the paired nasal bones, supported posteriorly by the nasal process of the frontal bone and laterally by the frontal processes of the maxilla (see Fig. 13.1). The nasal bones vary in length, constituting from one third to one half of the nasal framework. They are paired quadrilateral bones that are thick and narrow in their upper portion, becoming wider and thinner in the lower portion. The superficial surface is smooth and concave in the upper half and convex in the lower half. The inferior edge of the nasal bones is continuous with the upper lateral (triangular) cartilages, which extend underneath the nasal bones 4 to 7 mm (often called the keystone area).
External Nasal Cartilage Framework
The upper lateral (triangular) cartilages are paired structures that form the greater part of the middle one third of the lateral nasal wall (Fig. 13.1). Their medial borders fuse with the lateral expansions of the anterior border of the septal cartilage in its upper two thirds. In the lower one third, they are separated from the septum and are attached by intervening connective tissue. The upper border of the upper lateral cartilage inserts onto the deep surface of the inferior edge of the nasal bones for a few millimeters. The periosteum of the nasal bones becomes the perichondrium of the cartilage nasal skeleton at this junction. The lateral border of the upper lateral cartilage joins the piriform aperture of the maxilla. The inferior edge of the upper lateral cartilage slides under the lateral crus of the alar cartilage to which it is joined by a dense tissue, which is a prolongation of the superficial and deep perichondrial layers that include several fragments of cartilage called sesamoids. The attachment between the alar and upper lateral cartilages is often folded back by 2 to 3 mm and is frequently called the scroll area (see Fig. 13.2).
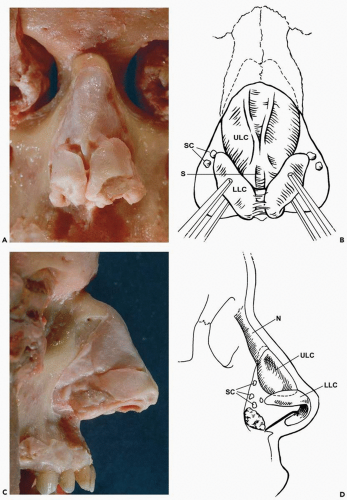
Figure 13.1 External skeleton of the nose. N, nasal bone; ULC, upper lateral cartilage; SC, sesamoid cartilages; S, cartilaginous septum; LLC, lower lateral cartilage.
|
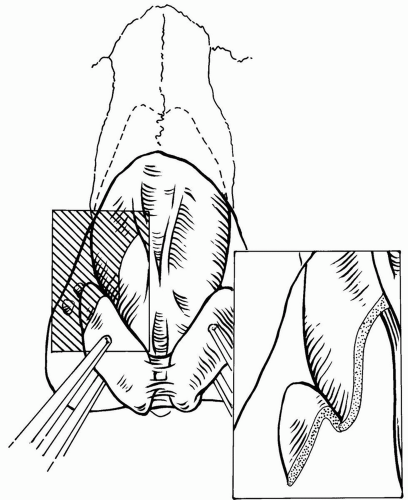
Figure 13.2 Scroll area where upper and lower lateral cartilages are joined by fibrocartilaginous tissue.
|
The alar (lower lateral) cartilages are paired structures that have medial and lateral crura. The two medial crura come together at the midline and take part in forming the columella (see Fig. 13.3). The posteroinferior edges of the medial crura diverge (foot plates) and attach to the septal cartilage by fibrous tissue. The lateral crura are quadrangular and usually convex. They contribute little to the shape or structure of the ala, which is primarily a fibrofatty structure. The length of the lateral crura varies considerably from one individual to another, but their outline is usually visible through the overlying skin. The lateral border of the lateral crura extends toward the piriform aperture but does not reach it being connected by intervening connective tissue and sesamoid cartilage islands (Figs. 13.1 and 13.2). The height of the lateral crura also varies widely, with a mean of approximately 11 mm. The superior edge of the lateral crura overlies the inferior edge of the upper lateral cartilage. The inferior border of the lateral crus does not follow the alar rim and is closer to the rim medially, where it may be 5 to 6 mm posterior. Laterally, the inferior edge of the lateral crus may be 12 to 14 mm superior to the alar rim (Fig. 13.1). Therefore, the inferior border of the lateral crus extends superiorly as it extends laterally. This relation is readily visible through the skin or by performing an endonasal examination with retraction of the alar rim. The junction of the medial and lateral crus can be abrupt, forming an acute angle, or genu. In some instances, a flat area is noted between them, giving rise to the term middle crus. The alar cartilages are attached by interdomal ligamentous attachments, which extend over the top of the cartilaginous septal angle, contributing to tip support (Fig. 13.3).
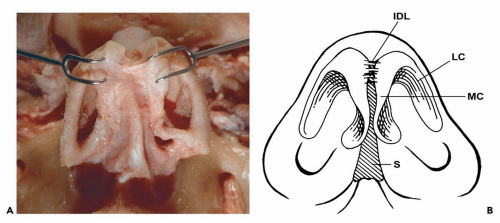
Figure 13.3 Base of the nose. IDL, interdomal ligaments; LC, lateral crus of the lower lateral cartilage; MC, medial crus of the lower lateral cartilage; S, septum.
|
The Nasal Septum
The septum of the nose is made of six structures; the septal crest of the maxilla, the perpendicular plate of the palatine bone, the perpendicular plate of the ethmoid bone, the vomer, the cartilaginous septum (quadrangular cartilage), and the membranous septum (see Fig. 13.4). The cartilaginous septum (quadrangular cartilage) is an anterior extension of the bony septum; it has a roughly quadrangular shape. The anterosuperior border contributes to the nasal bridge. In its upper one third, this border is located under the deep surface of the nasal bones. In its middle one third, it is in close relation to the upper lateral cartilages; the anterior septal border enlarges to form two lateral expansions that articulate with the medial borders of the upper lateral cartilages through a dense fibrous articulation. The anterior border of the septum is wide superiorly and narrows as it proceeds downward. The anterior septal angle is at the junction of the dorsal and caudal septa. In its lower one third, the septal cartilage is separated from the upper lateral cartilages and is clearly behind the alar cartilages. An anteroinferior border, extending obliquely posterior, forms a rounded angle with the anterior nasal spine to which it is firmly bound by the perichondrial and periosteal tissues that extend around it at this level to form a tight but somewhat mobile articulation. A posterosuperior border is joined to the perpendicular plate of the ethmoid by a tight attachment. The posteroinferior border extends obliquely from posterior to anterior. This flared border narrows posteriorly and has a caudal prolongation that extends between the ethmoid and the vomer. Anteriorly, the inferior border expands to install itself on the incisive crest that sometimes becomes a groove to hold this border.
Nasal Soft Tissues
The soft tissues covering the nose consist of skin, a complex musculoaponeurotic sheath, and the periosteum/perichondrium. The arteries and veins of the nose are in the soft tissues. Therefore, the plane of dissection in nasal surgeries should be close to the osteocartilaginous framework to avoid injuring these muscles and vessels. The nasal soft tissues are important in understanding the effect of certain surgical procedures on nasal function and esthetics. However, for the purpose of exposure of the nasal skeleton, these factors are less important because the dissection is made in the subperiosteal/subperichondrial plane.
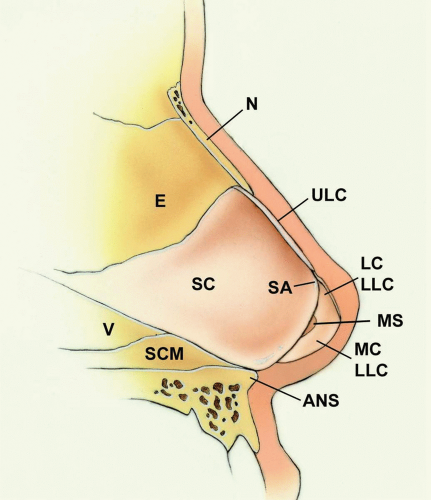
Figure 13.4 Components of the nasal septum. N, nasal bone; ULC, cut edge of the upper lateral cartilage; E, ethmoid; SC, septal cartilage; SA, septal angle; V, vomer; SCM, septal crest of the maxilla; LC, LLC, cut edge of the lateral crus, lower lateral cartilage; MS, membranous septum; MC, LLC, medial crus, lower lateral cartilage; ANS, anterior nasal spine.
|
TECHNIQUE
The external approach to the nasal skeleton involves only one external incision placed across the columella. This approach consists of bilateral marginal incisions connected by a transcolumellar incision. The soft tissue is elevated off the cartilages and nasal bones, exposing the entire tip and dorsum.
▶ Step 1. Vasoconstriction and Preparation
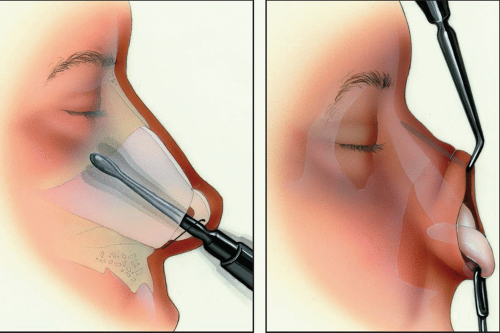
The vibrissae within the vestibules are shaved with a no. 15 scalpel or scissors and the nasal cavity is cleaned with a povidone-iodine solution. A combination of intranasal packs and vasoconstrictor injections can help with hemostasis during the surgery. Nasal packing with a vasoconstrictor (4% cocaine, 0.05% oxymetazoline, etc.) is placed along the length of the nasal floor, against the turbinates and under the osteocartilaginous roof. Local infiltration of a vasoconstrictor induces hemostasis and assists dissection by separating tissue planes. The infiltration is carried out between the skin and the osteocartilaginous skeleton, trying to deform the overlying skin as little as possible, and submucosally (see Fig. 13.5). After infiltration, gentle external pressure applied over the nose for 1 to 2 minutes helps spread the vasoconstrictor homogeneously, thereby reducing the external deformity. The external structures are then prepared in a standard manner.
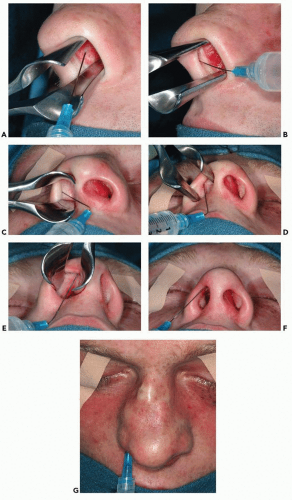
Figure 13.5 Photographs showing the injection of a vasoconstrictor to assist in hemostasis and develop a plane of dissection. A: Submucosal injection of the nasal septum; (B), injection of the membranous septum and along the medial crus of the lower lateral cartilage; (C-E), injection along the location of the marginal incision; (F), injection of the nasal dome; (G), injection just superficial to the upper lateral cartilages and the nasal bones.
Stay updated, free dental videos. Join our Telegram channelVIDEdental - Online dental courses
 Get VIDEdental app for watching clinical videos
Get VIDEdental app for watching clinical videos

|