Endonasal Approach
Several endonasal approaches and incisions to expose the nasal skeleton have been described. The technique for modification of the alar cartilages is the major variable in the different approaches. The endonasal approach described in this chapter is the “delivery approach” for exposing the lower lateral cartilages.
TECHNIQUE
▶ Step 1. Vasoconstriction and Preparation
The vibrissae within the vestibules are shaved with a no. 15 scalpel or scissors, and the nasal cavity is cleaned with povidone-iodine solution. A combination of intranasal packs and vasoconstrictor injections helps hemostasis during the surgery. Nasal packing with a vasoconstrictor (4% cocaine, 0.05% oxymetazoline, etc.) is placed along the length of the nasal floor, against the turbinates and under the osteocartilaginous roof. Local infiltration of a vasoconstrictor provides hemostasis and assists dissection by separating tissue planes. The infiltration is carried out between the skin and the osteocartilaginous skeleton, trying to deform the overlying skin as little as possible, and submucosally. After infiltration, gentle external pressure applied over the nose for 1 to 2 minutes helps spread the vasoconstrictor homogeneously, thereby reducing external deformity. The external structures are then prepared in the standard manner.
▶ Step 2. Cartilage Delivery Technique for Lower Lateral Cartilage Exposure
The alar cartilage delivery approach involves a marginal incision and an intercartilaginous incision connected to a partial or complete transfixion incision (see Fig. 14.1). The entire nasal skeleton can be exposed through these incisions, which are placed entirely within the nasal cavity.
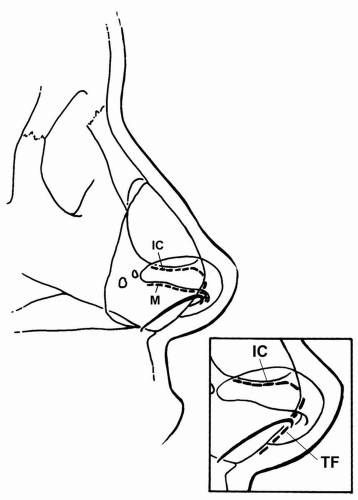
Figure 14.1 Incisions for the alar cartilage delivery approach. IC, intercartilaginous incision; M, marginal incision; TF, transfixion incision. Note how the transfixion incision follows the caudal border of the septal cartilage (inset).
|
A marginal incision for exposure of the dome and lateral crus should follow the free caudal margin of the lower lateral cartilage and not the margin of the nostril (see Figs. 14.1 and 14.2; see also Figs. 13.5, 13.6 and 13.7). Incisions should not be placed into the soft triangle—the portion of the nostril that is caudal to the alar cartilage. The soft triangle is formed by two juxtaposed layers of skin, unsupported by cartilage, with only loose areolar tissue between. Incisions in the soft triangle may result in disfiguring postoperative notching. This possible result is why the rim incision, which requires dissection through the soft triangle, is to be avoided.
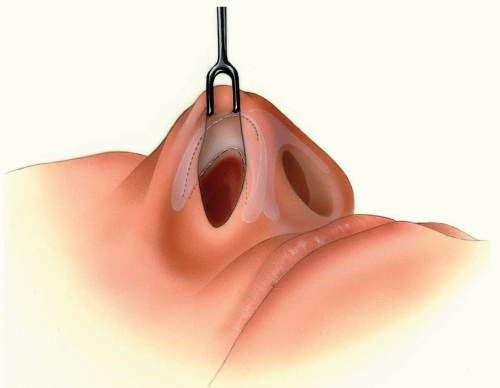
Figure 14.2 Retraction of the ala reveals positioning of the marginal, intercartilaginous, and transfixion incisions.
|
The nostril rim is retracted with a double skin hook and everted by placing the middle finger externally over the alar cartilage (Fig. 14.2). The caudal edge of the alar cartilage is identified through the vestibular skin. As described in Chapter 13, the inferior border of the lateral crus does not follow the alar rim, and is closer to the rim medially, where it may be 5 to 6 mm posterior to the alar rim. Laterally, the inferior edge of the lateral crus may be 12 to 14 mm superior to the alar rim. The inferior border of the lateral crus extends superiorly as it extends laterally (see Fig. 14.3). The back of the scalpel handle can be used to palpate the caudal border of the alar cartilage. An incision through the vestibular skin along the
contour of the alar cartilage is made to the depth of the cartilage (see Fig. 14.4). It begins laterally beyond the point where the caudal rim of the lateral crus diverges from the alar rim to turn cephalad, follows the rim medially to the apex and continues along the caudal rim of the medial crus, approximately 1 mm behind the rim of the columella, stopping at the columella-lobule junction. If required, it can be extended further inferiorly along the medial crus and more laterally along the lateral crus to facilitate delivery of the cartilage.
contour of the alar cartilage is made to the depth of the cartilage (see Fig. 14.4). It begins laterally beyond the point where the caudal rim of the lateral crus diverges from the alar rim to turn cephalad, follows the rim medially to the apex and continues along the caudal rim of the medial crus, approximately 1 mm behind the rim of the columella, stopping at the columella-lobule junction. If required, it can be extended further inferiorly along the medial crus and more laterally along the lateral crus to facilitate delivery of the cartilage.
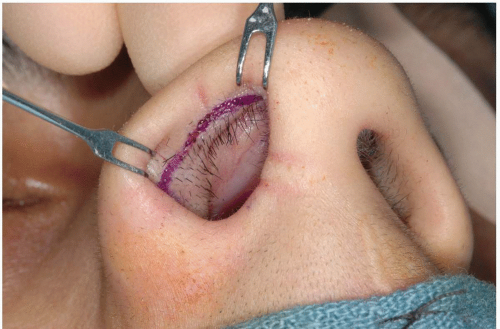
Figure 14.3 Photograph showing location of the marginal incision.
|
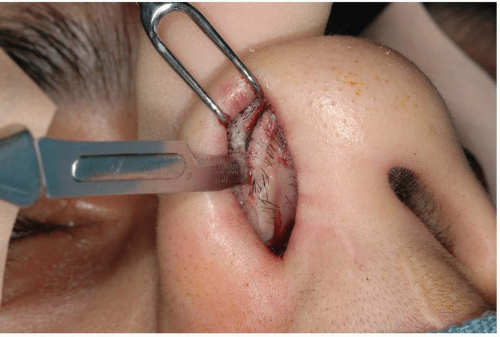
Figure 14.4 Photograph showing marginal incision being made. Note the skin hook retracting the alar rim superiorly while a finger placed outside the nose presses downward, facilitating the access.
|
The intercartilaginous incision (limen vestibuli incision) divides the junction of the upper and lower lateral cartilages (Figs. 14.1 and 14.2). The incision traverses the aponeuroticlike fibroareolar tissue that maintains the attachment between them (scroll area). The ala is retracted using a double skin hook and the inferior edge of the alar cartilage is identified. The skin hook elevates the alar cartilages, leaving the inferior edge of the upper lateral cartilage protruding into the vestibule, covered only by the nasal mucosa (see Fig. 14.5A). An incision is made along the inferior border of the upper lateral cartilage, beginning at the lateral end of the limen vestibuli and extending medially approximately 2 mm caudal and parallel to the limen (see Figs. 14.6A and B). It is important to make the incision 2 to 3 mm caudal to the limen vestibuli to avoid unnecessary scarring at the nasal valve area. The incision is then curved into the membranous septum anterior to the valve area, where
it meets the transfixion incision (Figs. 14.1, 14.2 and 14.6C). The length of the incision, which should always extend to the midline, varies with the extent of dorsum exposure necessary and alar cartilage to be freed during tip surgery.
it meets the transfixion incision (Figs. 14.1, 14.2 and 14.6C). The length of the incision, which should always extend to the midline, varies with the extent of dorsum exposure necessary and alar cartilage to be freed during tip surgery.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


