Introduction
White spot lesions are a common sequela of orthodontic therapy. In this parallel-group randomized trial, we assessed the effectiveness of 2 agents commonly used to ameliorate white spot lesions compared with a normal home-care regimen.
Methods
Patients aged 12 to 20 years were recruited from the offices of orthodontists and dentists who belonged to the Practice-based Research Collaborative in Evidence-based Dentistry network. The patients had their orthodontic appliances removed within the past 2 months and had at least 1 white spot lesion affecting their maxillary incisors. The subjects were randomized to 1 of 3 arms: (1) an 8-week regimen of MI Paste Plus (GC America, Alsip, Ill), (2) a single application of PreviDent fluoride varnish (Colgate Oral Pharmaceuticals, New York, NY), and (3) usual home care (control). Photographs were taken at enrollment and 8 weeks later. Two panels consisting of 5 dental professionals and 5 laypersons assessed the before-and-after pairs of photographs in a blinded fashion. Objective assessments and self-assessments were also performed.
Results
One hundred fifteen subjects completed the study; 34 were assigned to the MI Paste Plus group, 40 to the fluoride varnish group, and 41 to the control group. The mean improvements assessed by the professional panel were 21%, 29%, and 27% in the MI Paste Plus, fluoride varnish, and control groups, respectively.The results from the lay panel were 29%, 31%, and 25%, respectively. Objective improvements in the surface affected were 16%, 25%, and 17%, respectively; self-assessments of improvement were 37% in all 3 groups. No assessments indicated significant differences between subjects in the active arms compared with the control arm.
Conclusions
MI Paste Plus and PreviDent fluoride varnish do not appear to be more effective than normal home care for improving the appearance of white spot lesions over an 8-week period.
White spot lesions (WSLs), clinically defined as opaque, white areas caused by the loss of minerals below the outermost enamel layer, can be an unfortunate sequela of orthodontic treatment. Although prevention of these lesions is the goal of every orthodontist, the prevalence of WSLs after orthodontic treatment has been reported to be 5% to 97%. Once formed, WSLs compromise esthetics and can be extremely difficult or even impossible to reverse.
Saliva can remineralize WSLs to some degree, but this process is slow and rarely results in complete resolution of the lesions. The pattern of remineralization follows a time trend, with greater remineralization during the first few months and then continuing at a slower rate. Fluoride has been shown to increase the initial rate of remineralization. High doses of fluoride have been recommended during and after orthodontic treatment for arresting areas of decalcification and preventing WSLs from progressing to carious lesions. This should cause an increase in remineralization of the outer enamel and a decrease in demineralization of the inner enamel, resulting in a significant mineral gain. However, some authors warn against the use of high concentrations of fluoride because they believe this will cause remineralization mainly in the superficial part of the WSLs. This superficial layer might prevent calcium and phosphate from penetrating to the deeper layers of the enamel, thus inhibiting deeper remineralization and limiting the cosmetic improvement of the WSLs. Thus, the most ideal concentrations and delivery vehicles for fluoride remain controversial.
In recent years, MI Paste (GC America, Alsip, Ill) has often been prescribed for remineralization of WSLs. The active agent, casein phosphopeptide-amorphous calcium phosphate, is thought to stabilize and localize calcium, fluoride, and phosphate at the tooth surface in a slow-release amorphous form, thus enhancing deeper remineralization of WSLs. A number of in-vitro and in-situ studies have demonstrated the remineralizing potential of casein phosphopeptide-amorphous calcium phosphate. Recent studies have investigated the remineralization potential of casein phosphopeptide-amorphous calcium phosphate combined with fluoride and have found a synergistic effect when these are administered together. A newer product, MI Paste Plus (GC America), containing 900 ppm fluoride and casein phosphopeptide-amorphous calcium phosphate, is now commercially available.
Few in-vivo studies have investigated the effectiveness of remineralization products to address the appearance of WSLs after orthodontic treatment. With that in mind, we conducted this randomized trial of 2 commercially available products, MI Paste Plus and PreviDent fluoride varnish (Colgate Oral Pharmaceuticals, New York, NY), to assess their clinical effectiveness over an 8-week period.
Our objective was to compare the effectiveness of MI Paste Plus and PreviDent fluoride varnish (22,600 ppm of fluoride) with a standard oral hygiene regimen with toothpaste (1100 ppm of fluoride; Colgate Oral Pharmaceuticals) (control group) in improving the appearance of WSLs after orthodontic treatment. The results were (1) assessed by 2 blinded panels (expert panel and lay panel), using subjective measures; (2) assessed by 2 blinded examiners using objective measures; and (3) measured by the subjects’ self-assessments.
Material and methods
This was a randomized (1:1:1), single-blind, 3-armed, active-controlled, parallel-group trial. The trial was registered at ClinicalTrials.gov .
The study began in April 2010 in private orthodontic and general dentistry offices as part of the Practice-based Research Collaborative in Evidence-based Dentistry network (PRECEDENT). The network was operated jointly by the University of Washington and the Oregon Health and Science University, and it comprised a region of northwest states—Washington, Oregon, Montana, Idaho, and Utah—(NW PRECEDENT). The study was approved by the NW PRECEDENT Protocol Review Committee and the Human Subjects Review Committee at the University of Washington.
Eligible patients were recruited consecutively from the offices of NW PRECEDENT orthodontists and general dentists if they met the following eligibility criteria: completed fixed appliance orthodontic therapy within the past 2 months in the participating orthodontist’s or dentist’s office, had at least 1 WSL on the facial surface of a maxillary central or lateral incisor that was not present before orthodontic treatment (assessed with pretreatment photographs that were available as part of the routine initial records before orthodontic treatment), and were between the ages of 12 and 20 years. Exclusion criteria included unwillingness to be randomly assigned to 1 of the 3 treatment groups; any abnormal oral, medical, or mental condition (including any milk-related allergies and medical condition involving the kidneys); any therapy for WSLs after orthodontic treatment; any WSLs present on qualifying teeth with frank cavitation; and non-English speaking or non-English reading patients. Patients (and parents, if the patient was under 18 years old) consented before the start of the study.
The patients were randomly assigned in blocks of 3 or 6 to 1 of the 3 arms of the study.
- 1.
MI Paste Plus group (intervention). These patients received an 8-week supply of MI Paste Plus at the start of the study and instructions to apply a pea-sized amount to each arch twice daily. They also received the usual home-care oral hygiene instructions and a packet with nonprescription fluoride toothpaste (1100 ppm of fluoride), a manual toothbrush, and dental floss. Compliance was checked by questions at the follow-up visit about the frequency of application of the MI Paste Plus.
- 2.
Fluoride varnish group (intervention). These patients received 0.4 mL of 5% sodium fluoride varnish (22,600 ppm of fluoride, PreviDent) as a single application at the start of the study. They also received the usual home-care oral hygiene instructions and a packet with nonprescription fluoride toothpaste (1100 ppm of fluoride), a manual toothbrush, and dental floss.
- 3.
Home-care group (control). These patients received the usual home-care oral hygiene instructions and a packet with nonprescription fluoride toothpaste (1100 ppm of fluoride), a manual toothbrush, and dental floss.
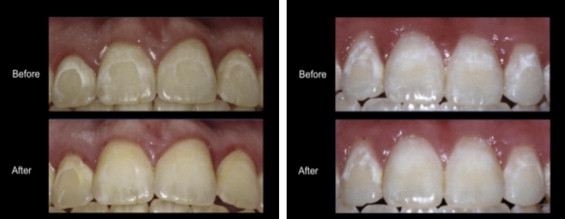
Each NW PRECEDENT provider and staff member completed study training before the enrollment of the patients. Calibration of the photographic protocols to standardize magnification, color, and shade was performed. Photographs were taken digitally as intraoral frontal views with the patient’s head tilted up approximately 5° to 10° to limit reflection from the flash to the incisal third of the maxillary incisors. Several digital photographs were taken at each time point to allow selection of the optimal image. The photographs ( Fig 1 ) were cropped to include only the 4 maxillary incisors, adjusted for brightness, color matched between sets, and saved in a 3000 × 1200 pixel 24-bit bitmap format with Photoshop (CS3 extended version 10.0.1; Adobe, San Jose, Calif). The NW PRECEDENT provider supervised all study-related activities, certified the accuracy of data collection, and authorized the data transmission. A baseline data form was completed during enrollment with the following information from the patient’s chart: length of the patient’s orthodontic treatment, date of removal of the orthodontic appliances, type of retainers used, oral hygiene status during treatment, and prior history of therapy to treat WSLs. The patient’s general or pediatric dentist was informed about his or her participation in the study and asked not to introduce any additional treatments for WSLs during the trial. Photographs were obtained when the intervention was begun and at follow-up 8 weeks later. If a patient was recruited on the day of removal of the fixed orthodontic appliances, the intervention photographs were delayed several days to coincide with the day of retainer delivery (typically 2-7 days after removal of the appliances). The rationale for delaying the intervention a few days was to allow resolution of gingival inflammation that might have masked portions of the WSLs and to allow the enamel to hydrate to physiologic levels after removal of the orthodontic adhesives. At the 8-week follow-up visit, the patient had posttreatment photographs and completed a questionnaire about satisfaction with the treatment, compliance, oral hygiene practices, and self-assessment of the percentage of improvement of the WSLs on a 100-mm visual analog scale. All data collection forms and photographs were uploaded through a secure online data transfer system maintained by the Axio Research Corporation (Seattle, Wash).
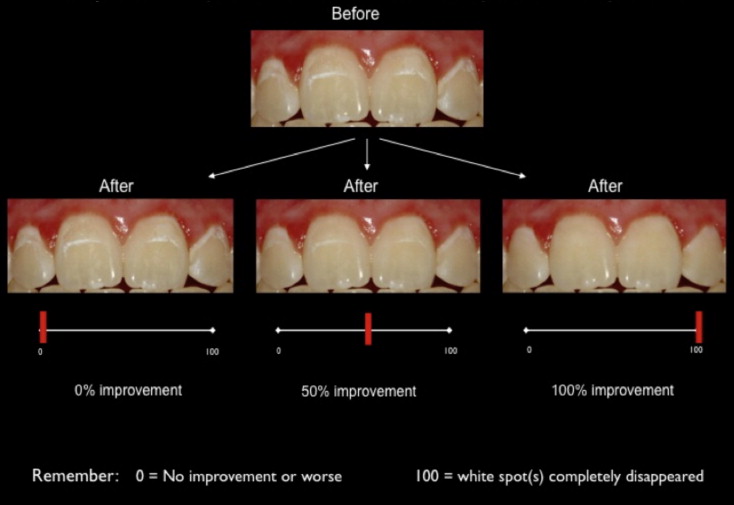
The primary outcomes with respect to the effectiveness of the MI Paste Plus and the PreviDent fluoride varnish were the mean percentages of improvement of the WSLs from entry to the 8-week follow-up with both subjective and objective assessments. For the subjective assessment, 2 blinded panels rated the improvement in WSL over the 8-week period using a visual analog scale. The first panel consisted of 5 dental experts (2 women, 3 men: 3 general dentists, 2 orthodontists). The second panel consisted of 5 laypersons (3 women, 2 men). The cropped and color-matched before-and-after images for each patient were imported into a PowerPoint (Microsoft, Redmond, Wash) slide with a black background. The raters then viewed these paired images on a laptop computer. To assist with calibration of the assessors, each examiner’s session began with instructions on the rating system, as well as several example sets of before-and-after images, altered in Photoshop to demonstrate improvements of 0%, 50%, and 100% ( Fig 2 ). The examiners evaluated the esthetic improvements of the paired images using the visual analog scale from 0 to 100 mm (0 mm, no improvement or worsened, to 100 mm, WSL completely disappeared). Each examiner performed the evaluation independently, and the order of the patients was shuffled to prevent bias from examiner fatigue. For each patient, the median value of the visual analog scores in each panel was selected to represent the percentage of improvement for that patient. For example, if the 5 examiners in the lay panel judged improvement to be 15%, 19%, 23%, 24%, and 35% for a particular patient, the median value for that patient would be 23%. To assess intraexaminer reliability, a random sample of 20 image pairs was selected for double evaluation by each rater with at least a week between evaluations.
Two examiners (a dental student and a general dentist) performed the objective assessments of the WSLs. Both were blinded to the treatment arms. They assessed the same initial and follow-up images used for the subjective assessments. These images were measured side by side to allow for exclusion of preexisting enamel variations and increase the examiner’s consistency and reliability. The WSLs and the total tooth surface area of the 4 maxillary incisors were outlined by using the “freehand selection” tool with a Genius MousePen 8 × 6 tablet (KYE Systems America, Miami, Fla) in the software program Image J (version 1.39; National Institutes of Health, Bethesda, Md). The total surface area of the WSLs of the 4 maxillary incisors was divided by the total surface area of the 4 maxillary incisors, and an average of the 4 teeth was calculated, resulting in the pretreatment and posttreatment proportions of WSLs relative to the total surface area of the 4 incisors. The change in percentage of the area affected was obtained by subtracting the posttreatment proportion from the pretreatment proportion. When this resulted in a negative value (ie, the percentage of the area of the affected teeth appeared to increase for a subject), a value of zero was assigned to the change score to standardize the scale used in the objective and subjective assessments. The same 20 sets of duplicates used in the subjective assessment were measured side by side a week apart to determine intraexaminer reliability.
An a-priori power analysis was conducted to determine the required number of patients to assess the influence of the 2 treatments on the reduction of WSLs. Data from 2 studies provided estimates of standard deviations of percentage changes in lesion size directly after fixed orthodontic appliance removal. The average percentage of reduction in WSL area was 50% (SD, 27%). Time course curves in both articles appeared to indicate that the reductions at 26 and 52 weeks, respectively, would be 20% greater than the reduction at 8 weeks, the length of the follow-up for this study. At a sample size of 120 subjects, the study was calculated to have good power (80%) to detect a 20% difference in WSL improvement on the visual analog scale, if the standard deviation was 25%. These estimates assumed a 10% loss to follow-up and nominal significance levels of 0.025 for each between-group comparison.
The randomization sequence was created by using statistical software (Axio Research) and was stratified by each office by using random block sizes of 3 and 6. The random block sizes were used to prevent practitioners from guessing patient assignments. The allocation sequence was concealed from the office during enrollment, and patients were consecutively enrolled as inclusion criteria were met. After informed consent was obtained and baseline enrollment forms were completed, the NW PRECEDENT office phoned Axio Research to receive the patient’s treatment assignment.
NW PRECEDENT providers, staff, and patients were aware of their allocated arm, but the outcome assessors and the study investigators were kept blinded to the study arms until completion of the statistical analyses.
All patients in the study received their assigned treatment and a small gift for participating in the study. A data safety monitoring board, composed of persons not directly involved in patient care or data collection, periodically reviewed accumulated data for evidence of adverse or beneficial treatment effects, a need for modification of study protocols, and assessment of data quality and clinic performance.
Statistical analysis
Analyses were conducted by using SAS software (version 9.2; SAS Institute, Cary, NC) on a Windows operating system (Microsoft).
Demographic data were summarized by using frequency tables with 95% confidence intervals for proportions.
The first aim was to compare the active treatments (MI Paste Plus, PreviDent fluoride varnish) with the control (standard oral hygiene with fluoride toothpaste) in their overall WSL percentages of improvement (ie, the mean of the medians of the visual analog scores). Expert and layperson scores were considered to be separate outcomes. Therefore, this aim comprised 2 hypothesis tests for each type of assessment with a significance threshold of an alpha of 0.025 for each comparison: no difference between active treatment and control in median expert visual analog scale ratings, and no difference between active treatment and control in median layperson visual analog scale ratings.
The second aim compared the objective assessment of WSL improvement: no difference between active treatment and control in the objective ratings.
The third aim compared the patient’s self-assessment of improvement: no difference between active treatment and control in self-assessed improvement.
The analyses for the aims were performed by using a linear regression model, accounting for possible effects associated with age, sex, and initial WSL severity. The methods of generalized estimating equations were incorporated into these models to account for possible correlations between patients from the same orthodontic practice. The effect of interest was the mean percentage of improvement over 8 weeks.
Results
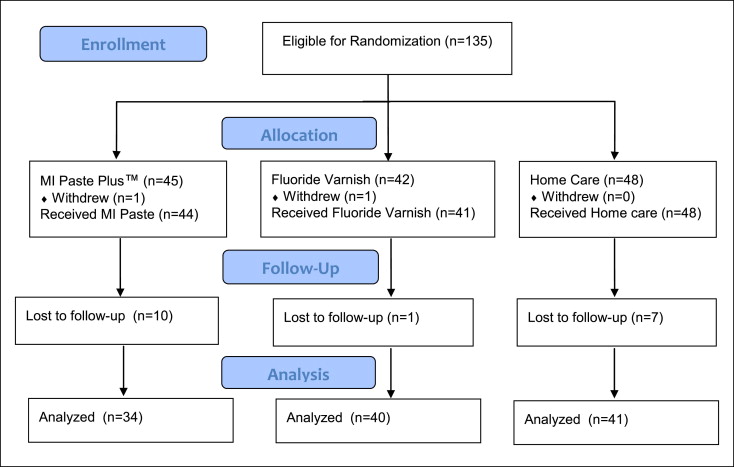
A total of 135 patients were eligible for randomization into the study ( Fig 3 ). Twenty participants withdrew or were lost to follow-up between the start and the end of the study, including 11 from the MI Paste Plus group, 2 from the PreviDent group, and 7 from the home-care control group. They did not vary with respect to demographic data and initial WSL severity compared with the subjects who completed the study.
Using the 20 sets of duplicate measurements, the intracluster correlation coefficients for the lay panel, the expert panel, and the objective raters were 0.71, 0.72 and 0.85, respectively, indicating good reliability.
A total of 115 participants (56 boys, 59 girls; mean age, 14.4 ± 1.5 years) finished the study and had complete records for analyses. The primary analysis was intention to treat and involved all patients who were randomly assigned. The 3 groups were well matched in all characteristics at enrollment ( Table I ). Of the 115 subjects, 34 received MI Paste Plus, 41 received PreviDent, and 40 received no active treatment.
| Treatment group | ||||
|---|---|---|---|---|
| MI Paste Plus ( n = 34) | PreviDent fluoride varnish ( n = 40) | Home care ( n = 41) | All ( n = 115) | |
| Age (y) | 14.6 (1.4) | 14.4 (1.5) | 14.3 (1.5) | 14.4 (1.5) |
| Female | 15 (44%) | 23 (58%) | 21 (51%) | 59 (51%) |
| Race/ethnicity | ||||
| Non-Hispanic white | 19 (56%) | 23 (58%) | 25 (61%) | 67 (58%) |
| Other or multiple race | 6 (18%) | 3 (8%) | 4 (10%) | 13 (11%) |
| Unreported | 9 (26%) | 14 (35%) | 12 (29%) | 35 (30%) |
| Number of teeth affected by WSL (1-4) | 3.3 (1.0) | 3.2 (0.9) | 3.2 (1.1) | 3.2 (1.0) |
| Initial surface area affected by WSL (%) | 11.8 (8.6) | 11.2 (6.2) | 11.5 (9.6) | 11.5 (8.2) |
| Oral hygiene level (based on latest toothbrushing and flossing habits) (%) | ||||
| Good | 3 (9%) | 2 (5%) | 5 (12%) | 10 (9%) |
| Fair | 15 (44%) | 18 (45%) | 14 (34%) | 47 (41%) |
| Poor | 16 (47%) | 20 (50%) | 22 (54%) | 58 (50%) |
| Weeks from orthodontic appliance removal to enrollment | ||||
| Mean (SD) | 1.03 (1.8) | 0.93 (1.7) | 1.5 (2.3) | 1.2 (2.0) |
| ≤1 week (%) | 24 (71%) | 31 (78%) | 27 (66%) | 82 (71%) |
| Weeks from baseline to follow-up photograph | 9.5 (4.6) | 9.6 (3.0) | 11.0 (6.8) | 10.1 (5.1) |
∗ For the continuous variables, the values reported are means (and standard deviations). For categorical variables, count (%).
The mean improvements assessed by the expert panel were 21%, 29%, and 27% in the MI Paste Plus, PreviDent, and home-care control groups, respectively ( Table II ). The results from the lay panel were 29%, 31%, and 25%, respectively. The objective improvement scores were 16%, 25%, and 17%, and the self-assessed improvement scores were 37% in all 3 arms. Differences with 95% confidence intervals between the active treatment groups and the control group, after adjustment for Dental Practice-based Research Network office, age, sex, and WSL severity, are presented in Table III . No statistically significant differences were observed when comparing either active group with the control group. The differences in adjusted improvement between the active treatment groups and the control group did not differ by more than ± 6% for any comparison. The estimates of intracluster correlation coefficients for the various types of assessment within practices were the following: expert judges, 0; lay judges, 0.01; objective assessment, 0; and self-assessment, 0.23.


