Introduction
The aim of this study was to compare the effects of a nonconventional elastomeric ligature (Slide; Leone, Florence, Italy) with those of a conventional elastomeric ligature (Ormco, Orange, Calif) on microbial flora and periodontal status in orthodontic patients.
Methods
A total of 13 orthodontic patients scheduled for fixed orthodontic treatment were selected for this study. The use of Slide and conventional elastomeric ligatures in fixed orthodontic appliances was tested. Microbial and periodontal records were obtained before bonding and 1 and 5 weeks after bonding. For the statistical analysis and calculations, SPSS software (version 15.0; SPSS, Chicago, Ill) was used. In the statistical decisions, P <0.05 values were accepted as significantly different.
Results
No significant differences between Slide and conventional elastomeric ligatures were evident at 1 week or 5 weeks after bonding, with regard to gingival index, plaque index, gingival bleeding index, or pocket depth scores ( P >0.05). Similarly, aerobic and anaerobic bacteria counts did not differ significantly on the surface or on the elastics ( P >0.05).
Conclusions
Although the Slide ligatures cover the total surface of the bracket, they do not cause significantly more plaque accumulation or periodontal problems than do the conventional elastomeric ligatures.
Maintaining daily oral hygiene can be difficult after the placement of orthodontic brackets and bands because they can prevent toothbrushes and floss from efficiently cleaning the proximal and buccal surfaces of teeth. Pathologic changes including gingival inflammation, bleeding, gingival hyperplasia, and increase in pocket depth have been reported in patients receiving orthodontic treatment. It has also been reported that the plaque-retaining characteristics of orthodontic appliances are responsible for the development of periodontal disease.
Nonconventional elastomeric ligatures (Slide; Leone, Florence, Italy) are a recent development in orthodontics and are manufactured using a special polyurethane mix and injection molding. Their potential applications are similar to those of conventional elastomeric ligatures; however, when fixed to the bracket and archwire, the ligature’s shape allows the wire to slide through a tube-like slot with less resistance. Friction is reduced, increasing patient comfort and potentially reducing treatment time. However, because the Slide ligatures cover the entire surface of the bracket, we investigated whether this was associated with an increase in plaque accumulation.
To our knowledge, there are no reported studies of plaque accumulation on Slide ligatures, although some studies have reported reductions in friction force resulting from their use. The aims of this prospective study were to compare Slide ligatures with conventional elastomeric ligatures (Ormco, Orange, Calif) in fixed orthodontic appliances with regard to subgingival microflora and to assess the effect on periodontal tissues of potential differences between them in this respect.
Material and methods
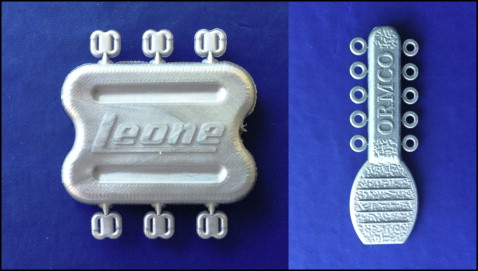
A total of 13 orthodontic patients (10 girls, 3 boys; mean age, 16.2 years) in the Department of Orthodontics of Gulhane Medical Academy in Ankara, Turkey, were chosen randomly, and each patient provided written informed consent. The study protocol was approved by the research ethics committee of the university. All patients were Class I and right-handed, had their permanent dentition, were free of dental plaque, and received professional guidance on oral hygiene (Bass technique) and prophylactic treatment 10 days before the baseline examination. Inclusion criteria for the patients were a healthy systemic condition, no use of anti-inflammatory drugs or antibiotics during the 3 months before the study, probing depth throughout the dentition not exceeding 4 mm, attachment loss at any interproximal site not exceeding 2 mm, no radiographic evidence of periodontal bone loss, and no mouth breathing. Patients were given a standard toothpaste and asked to refrain from using any other oral hygiene products for the duration of the study. Two elastomeric ligatures (Slide and conventional elastomeric) were used to fix the archwires ( Fig 1 ). Straight-wire appliances (0.18 in) were bonded to the maxillary teeth from the first molar to the contralateral first molar, and a 0.12-in nickel-titanium alloy archwire was used for initial leveling. There were 2 groups of teeth in the study, differing with respect to ligation material. Group 1 comprised 13 maxillary left first premolars ligated with Slide ligatures, and group 2 comprised 13 maxillary left second premolars ligated with conventional elastomeric ligatures. Microbial counts and periodontal measurements were determined for both groups.
Microbial and periodontal records were obtained before bonding and 1 week and 5 weeks after bonding. The gingival index, plaque index, gingival bleeding index values, and pocket depth values were recorded from the second premolars by the same examiner (H.A.), who was calibrated before the study. At each appointment, the ligatures and archwires were carefully removed. The experimental areas were isolated with sterile cotton rolls to prevent contamination by saliva. The samples of the biofilm, 2 mm supragingivally and 2 mm subgingivally, were obtained from the maxillary left first and second premolars using a sterilized periodontal curette and placed in an Eppendorf tube containing 1 mL of liquid transport medium. Serial 10-fold dilutions of the transport medium that contained the sample of plaque were prepared to 10 −4 , and 100 μL of the diluted samples were inoculated on blood agar and brucella agar (Oxoid; Thermo Scientific, Basingstoke, Hampshire, England). These plates were incubated for 48 hours at 37°C, with 1 plate in aerobic conditions and the other in anaerobic conditions (GasPak; Becton Dickinson Microbiology Systems, Cockeysville, Md).
The total numbers of the colony-forming units were determined on the basis of serial dilutions from 10 −5 to 10 −7 on the media. All of this process and colony counting were done by the same technician (S.D.) in the Department of Microbiology.
Statistical analysis
A power analysis established by G*Power software (version 3.1.3; Franz Faul, University of Kiel, Kiel, Germany) showed that the total sample size of 26 provided more than 78% power to detect significant differences with an effect size of 0.5 between the 2 measurements at a significance level of 0.05.
The normality of the distribution of index values and bacteria measurements was assessed using the Shapiro-Wilks test. No variable had a normal distribution; thus median values (interquartile range) were used as the descriptive statistics. For comparisons between the initial index values, Mann-Whitney and Kruskal-Wallis nonparametrical variance analyses were used. For the comparison of values measured at 1 and 5 weeks, surface elastic bacterial counts of every bacterial species investigated according to time and group were compared using the Wilcoxon matched-pairs signed rank test. All statistical analyses and calculations were performed with SPSS for Windows software (version 15.0; SPSS, Chicago, Ill). With regard to interpretation of the statistical analyses, P <0.05 was deemed to indicate statistical significance.
Results
Before the intervention, the gingival, plaque, and gingival bleeding indexes, the pocket depth values, and the intraoral surface bacterial counts of the conventional and Slide ligature groups were quantified. Before treatment, there were no significant differences in any values between the groups with regard to any of the 4 surfaces of the teeth (mesial, distal, palatal, buccal). Similarly, aerobic and anaerobic bacteria counts in the 2 groups did not differ significantly before treatment.
The same variables that were evaluated before treatment were reevaluated at 1 week and 5 weeks after treatment. No statistically significant differences between the groups were evident for any of the gingival index values investigated ( P >0.05). Moreover, no statistically significant differences between these groups were evident for the plaque index values for any of the 4 surfaces investigated ( P >0.05). The gingival bleeding index values of the 2 groups did not differ significantly for any of the 4 surfaces investigated ( P >0.05).
No statistically significant differences were evident between the groups with respect to the pocket depth values of any of the 4 surfaces investigated ( P >0.05). No statistically significant differences between the 2 groups were evident ( P >0.05) with respect to the aerobic and anaerobic surfaces and elastic bacterial counts 1 week after intervention.
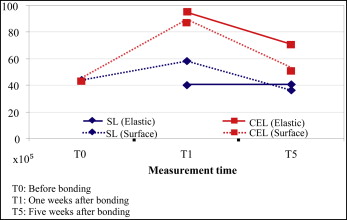
No significant differences between the 2 groups were evident at 5 weeks with regard to the gingival, plaque, and gingival bleeding indexes and the pocket depth scores ( P >0.05). Similarly, the aerobic and anaerobic bacterial counts did not differ significantly with respect to the surfaces or the elastics ( P >0.05). The elastics showed similar features at 1 week and 5 weeks. Surface and elastic aerobic and anaerobic bacterial count medians are shown in Figures 2 and 3 . Surface bacteria counts obtained from the 2 groups at the different time points did not differ significantly ( P >0.05) ( Figs 4 and 5 ).