Introduction
The purpose of this study was to determine the skeletal, dental, and soft-tissue changes in response to camouflage Class III treatment.
Methods
Thirty patients (average age, 12.4 ± 1.0 years) with skeletal Class III malocclusions who completed comprehensive nonextraction orthodontic treatment were studied. Skeletal, dental, and soft-tissue changes were determined by using published cephalometric analyses. The quality of orthodontic treatment was standardized by registering the peer assessment rating index on the pretreatment and posttreatment study models. The change in the level of gingival attachment with treatment was determined on the study casts. The results were compared with a group of untreated subjects. Data were analyzed with repeated measures analysis and paired t tests.
Results
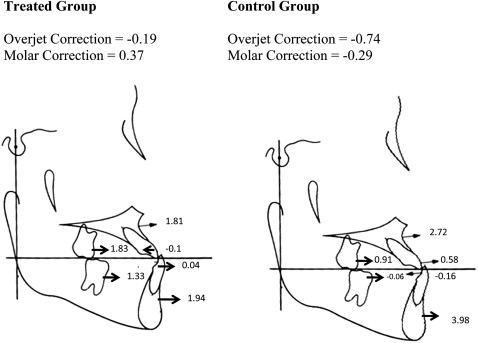
The average change in the Wits appraisal was greater in the treated group (1.2 ± 0.1 mm) than in the control group (–0.5 ± 0.3 mm). The average peer assessment rating index score improved from 33.5 to 4.1. No significant differences were found for the level of gingival attachments between the treatment and control groups. The sagittal jaw relationship (ANB angle) did not improve with camouflage treatment. A wide range of tooth movements compensated for the skeletal changes in both groups. The upper and lower limits for incisal movement to compensate for Class III skeletal changes were 120° to the sella-nasion line and 80° to the mandibular plane, respectively. Greater increases in the angle of convexity were found in the treated group, indicating improved facial profiles. Greater increases in length of the upper lip were found in the treated group, corresponding to the changes in the hard tissues with treatment.
Conclusions
Significant dental and soft-tissue changes can be expected in young Class III patients treated with camouflage orthodontic tooth movement. A wide range of skeletal dysplasias can be camouflaged with tooth movement without deleterious effects to the periodontium. However, proper diagnosis and realistic treatment objectives are necessary to prevent undesirable sequelae.
Editor’s summary
Every time I examine a patient with complete anterior crossbite, I ask myself the same question. “What are the limitations to successfully treating this patient without surgery?” The earlier I focus on the limitations of camouflage treatment, the more pleased I seem to be with the final outcome. But what characteristics should we look for when considering Class III nonsurgical treatment? The prevalence of Class III malocclusion in the United States is about 1%, but nearly 16% of the patients referred to orthodontists between the ages of 4 and 10 have Class III problems. The strategy for camouflage treatment usually involves proclination of the maxillary incisors and retroclination of the mandibular incisors to improve the occlusion as well as to correct the underlying skeletal problem. Although these changes can be accomplished with a chincap to the mandible or a protraction facemask to the maxilla, few studies describe the range of tooth movements that can alter this type of malocclusion without leaving the occlusion in an unstable relationship. The objective of this investigation was to determine the skeletal, dental, and soft-tissue changes that occur in response to camouflage Class III treatment.
The records of 30 patients (age, 12.4 years) were selected from the files of an author for study. All had completed Class III camouflage treatment over an average of 2 years 2 months. A control group of 30 children, matched by age, sex, and craniofacial morphology, was also identified. Read this entire article online to become familiar with the number of variables compared from all available pretreatment and posttreatment orthodontic records. As a result of early treatment, the changes were 2 to 8 mm in the maxillary base and 3 to 9 mm in the mandibular base in both the treated and control groups. Similar distributions were seen in both groups. The changes in mandibular incisor inclination were –10° to 15° in the treated group and –10° to 6° in the control group. The changes in maxillary incisor inclination were –6° to 12° in the treated group and –3° to 12° in the control group. No significant differences were found in molar relationships between the changes in the treated group compared with the control group.
Camouflage treatment did not improve the sagittal jaw relationships. In fact, the jaw relationship became worse with treatment because of the disproportional growth of the maxilla and the mandible. In addition to other changes with additional growth, the average loss of gingival attachment in the treated group was similar to that in the control group. When treating patients of this type of problem, clinicians must monitor their growth to determine whether they grow out of the range of successful camouflage treatment. In concluding remarks, the authors noted, “Most differences were attributed to tooth movement to reduce dental compensation of the skeletal malocclusion and improve the facial profile. The range of skeletal and dental changes in response to orthodontic treatment suggests that much skeletal dysplasia can be successfully camouflaged with tooth movement without deleterious effects to the periodontium.” Because long-term records are not yet available for this treatment group, caution is advised in assuming the permanency of acceptable outcomes at this time. Proper diagnosis and the establishment of realistic treatment objectives by the clinician and the patient are necessary to prevent undesirable sequelae in Class III camouflage treatment.