Unfortunately, few of these issues are or can be addressed by distractors that are commercially available today. Extraoral distractors, especially those applied to the mandible, are relatively easy to apply but have a variety of issues, including pin tracts and early mobility of pins ( Fig. 1 ). Because of the distance from the bone and flexion of the pins, the amount of movement achieved with each turn of the distractor is not as exact as that seen with distraction devices applied intimately to the bone. Multivector extraoral distractors allow change in the primary vector of distraction as opposed to internal distractors where it is much more complicated to change the primary vector. Although continuously activated distractors have been developed for laboratory use, those available for clinical use require manual activation two or more times a day to achieve the desired rate and rhythm of distraction. This manual component to activation requires that patients be educated as to how and why the appliance the appliance is used. Follow-up visits often are required to assure that patients or their family members are using an appliance correctly.

The further away from the ideal center of distraction an appliance is placed, the more asymmetric the movement of the segments. The classic example of this is when a surgically assisted rapid palatal expansion is done ( Fig. 2 ). The appliance is cemented to the teeth, yet the ideal point for attachment is to the middle of the palatal tissue. Because of the position of the distractor, when it is activated, there is more expansion at alveolar portion of the maxilla and less at the apex of the palate ( Fig. 3 ). In addition, the rotation of the segments causes the palatal cusps of the upper molars to occlude with the lower molars with a resultant anterior open bite. Bone-born appliances currently used in Europe to expand the maxilla do not have this problem ( Fig. 4 ).



Midface and maxilla
Submerged versus nonsubmerged
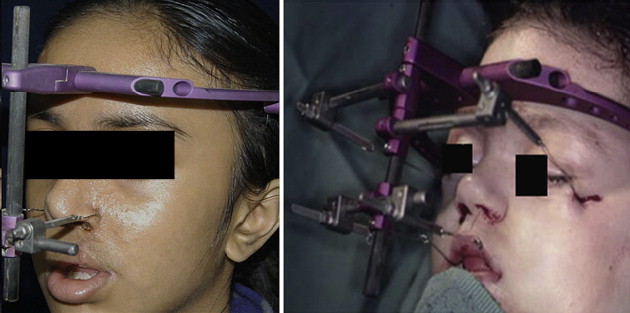
The basic distractor is a tram that allows expansion in one or more directions that has some sort of attachment to the bone, teeth, or both ( Fig. 5 ). Submerged distractors have a port that emerges through the mouth or transcutaneously ( Fig. 6 ). Nonsubmerged are extraoral and attached directly to the bone or teeth. Whether or not the mandible or the maxilla is addressed, the desired movement of segments is seldom in one direction. To change the primary extrinsic vector, the distractor needs multiple options or a second extrinsic vector, such as elastics, applied to appliances on the teeth. Midfacial advancement at the Le Fort III level and frontofacial advancements can be approached with internal or external devices depending on the circumstances. The internal devices usually are placed at the level of the body and arch of the zygoma in order to obtain true advancement of the midface rather than pivoting at the incisor region or the nasal root region ( Fig. 7 ). Extraoral distractors used to move the maxilla or combinations of the maxilla and upper parts of the face allow the greatest opportunities to change the primary vector of distraction ( Fig. 8 ). The wires used for the distraction can stretch the first few days and may not be a true indicator of advancement if the activation is based on turns of the distraction device alone. Extraoral distractors generate a moment arm caused by the point of attachment to the segment and the design of the osteotomy. With an external distractor, the vector can be modified by changing the position of appliance of the rod. When this is done during distraction, however, increase or decrease in the tensional forces placed on the maxilla must be considered. For example, if the appliance is moved inferiorly, tensional forces increase, whereas the reverse is true when it is moved upward. Attachments for activating wires can be to the appliances fabricated to fit the teeth and directly to the bone (for more information see the article by Reddy and Elhadi elsewhere in this issue).