Introduction
In this study, we examined displacement (labiopalatal and mesiodistal) and angulation of unerupted permanent maxillary canines on either side in children (n = 49) aged between 10 and 12 years with unilateral absence of the canine bulge on palpation.
Methods
The side without the canine bulge was considered the experimental (n = 49) and the contralateral side (where the bulge was palpable) the control (n = 49) in each subject. Orthopantomographs were taken to assess mesiodistal displacement and angulation of the canines on both sides. The horizontal tube shift method was used to assess the labiopalatal displacement of the canines on the experimental sides.
Results
There was a significantly high possibility of finding mesially overlapping canines (with respect to the lateral incisor on the orthopantomograph) on the sides without the bulge (chi-square, 60.05; P <0.001), all of which were found to be palatally displaced. However, 22.45% of the canines on the side without the bulge showed no abnormal displacement. The mean angulation was lower for palatally displaced canines than those that were not ( t = 9.89; P <0.001).
Conclusions
There is a significantly high possibility of finding palatally displaced canines in children aged 10 to 12 years on sides with the canine bulge absent on palpation; rarely, the canine is transposed with the first premolar. Palatally displaced unerupted canines have a significantly high possibility of being more mesially angled (to the horizontal) on the orthopantomograph compared with undisplaced canines.
The maxillary permanent canine is a frequently displaced tooth in the dental arch, second only to the third molars in frequency of impaction. Moss observed that frequently displacement is due to its high developmental position and the advanced state of development of its crown at an early age.
The reported prevalence of palatally displaced canines ranges from 0.8% to 2.8%. It is predominantly a European trait, occurring 5 times more frequently in Europeans than in Asians.
The exact etiology of palatally displaced canines is unknown; however, 2 common theories might explain the phenomenon: the guidance and the genetic theories. The guidance theory, in its simplest form, regards the distal aspect of the lateral incisor root as the guide to allow the canine to move safely into position. If the lateral incisor is anomalous or missing, this guidance is lost, resulting in palatal displacement of the canine. The genetic theory focuses on other dental abnormalities such as tooth size, shape, number, and structure, which are linked genetically.
Crowding or lack of space in the arch usually results in buccal displacement. Jacoby, however, noted that, in 85% of palatal impactions, there was adequate space for the eruption of the canine.
A bulge is normally palpable high in the alveolar process above the deciduous canine. Since the canines are palpable from 1 to 1.5 years before they emerge, the absence of the canine bulge after the age of 10 years is a good indicator that the tooth is displaced from its normal position, and ectopic eruption or impaction is a future possibility.
This study was done to assess the labiopalatal displacement, sector location, and internal mesial angulation of unerupted permanent canines on the sides without the canine bulge unilaterally and to compare these parameters with canines on the contralataral sides where the bulge was palpable.
Material and methods
Children visiting the Department of Pedodontics and Preventive Dentistry at Christian Dental College in India were analyzed for the following criteria: (1) age between 10 and 12 years (chronologic); (2) maxillary incisors erupted; (3) maxillary permanent canines unerupted; (4) healthy, with no syndromes or previous illnesses that would have interfered with the formation or eruption of permanent teeth; (5) no history of extraction of the maxillary deciduous canines (if they were missing, it was solely due to natural exfoliation); and (6) unilateral absence of a palpable maxillary canine bulge.
The first 49 children (28 boys, 21 girls) who fulfilled those criteria constituted the study sample.
The presence or absence of the bulge was confirmed for each subject by digital palpation on the alveolar process and the vestibule extending from the distal aspect of the deciduous canine (or from the mesial aspect of the deciduous first molar or first premolar if the deciduous canine had exfoliated) until the distal aspect of the permanent lateral incisor on the labial side with the index finger of the right gloved hand on both sides by 1 examiner (P.C.).
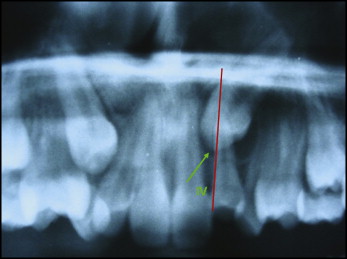
The side without the canine bulge on palpation ( Fig 1 ) was considered the experimental side, and the contralateral side where the bulge was palpable ( Fig 2 ) was considered the control side in each subject. Therefore, 49 experimental sides were compared with 49 control sides.


The permission of the Ethical and Research Committee of Christian Dental College was obtained before the study.
An orthopantomograph (OPG) was taken for each subject after obtaining informed written consent from the parents.
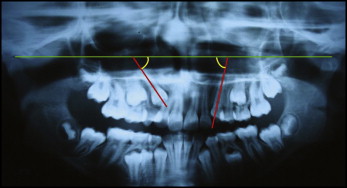
Each OPG was evaluated for the following: (1) the mesiodistal orientation of the maxillary permanent canine on the experimental and control sides, (2) angulation values (mesial) between the long axis of the canines and the constructed horizontal for both sides, and (3) the presence of any supernumerary teeth, odontomas, tooth transpositions, and other pathologies.
All OPGs were taken with the same panoramic radiograph machine (Rotograph Plus, Villa System Medical, New York, NY) with standardized settings for all the exposures. The developing and fixing times were standardized for all OPGs.
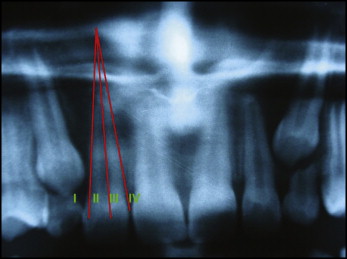
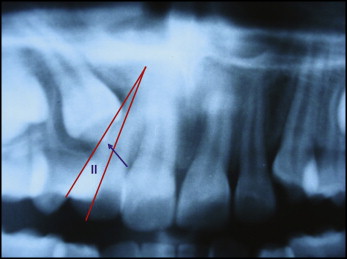
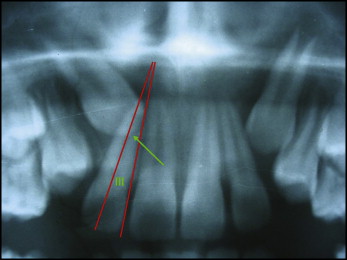
The mesiodistal orientation of the canine with respect to the maxillary permanent lateral incisor was evaluated by the sector method of Lindauer et al ( Fig 3 ). The canine cusp tip was related to the lateral incisor root on the OPG by one of the following sectors by 1 examiner. Sector I was the area distal to a line tangent to the distal heights of contour of the lateral incisor crown and root ( Fig 4 ). Sector II was mesial to sector I but distal to a line bisecting the mesiodistal dimension of the lateral incisor along the long axis of the tooth ( Fig 5 ). Sector III was mesial to sector II but distal to a line tangent to the mesial heights of contour of the lateral incisor crown and root ( Fig 6 ). Sector IV included all areas mesial to sector III ( Fig 7 ).
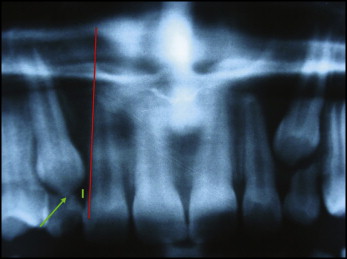
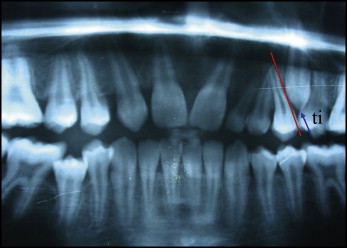
Two subjects in this study had canine cusp tips that could not be classified into any sector defined by Lindauer et al. Both had congenitally missing maxillary lateral incisors, bilaterally. One of them also had a canine-first premolar transposition on the experimental side. Therefore, 2 more sectors were created and used: sector i, where the location of the maxillary permanent canine cusp tip could not be compared with the lateral incisor because of congenital absence of the lateral incisor ( Fig 8 ); and sector ti, where the maxillary permanent canine cusp tip was distal to the first premolar, with congenital absence of the lateral incisor on that side ( Fig 9 ).

The mesiodistal locations of the canine cusp tips were recorded for both the experimental and the control sides by using the above 6 sectors and compared.
The sector locations of the canines from each OPG were evaluated by the same examiner 3 times at weekly intervals to confirm the findings.
The labio-palatal orientation of the canine cusp tips with respect to the lateral incisors on the experimental sides (sector I, II, III, or IV) was evaluated by using the horizontal tube shift method (with 2 intraoral films). The evaluation was done 3 times from the intraoral films at weekly intervals by 1 examiner. However, the labio-palatal orientation of the canines in sectors i and ti could not be considered for evaluation because of the congenital absence of the lateral incisors for comparison.
The angulations were measured for the canines in sectors I, II, III, and IV for comparisons between angulations of canines in sector I (n = 60) and those in sectos II, III, and IV (n = 36). The method used was similar to that of Warford et al.
The angular measurements were made on acetate paper positioned on the OPG that was placed over the radiograph viewing box. The most superior point of the condyle was selected as a landmark. A bicondylar line was then drawn and used as a constructed horizontal reference line. The measurement was taken of the mesial angle formed by using the constructed horizontal and the long axis of the canine ( Fig 10 ). The angular values were recorded 3 times at weekly intervals by the same examiner, and the mean of the 2 closest angular measurements was taken as the final reading.