Introduction
Some chronic diseases are associated with changes in the morphology of sella turcica, and type 1 diabetes is the most common chronic disease in children and adolescents. Therefore, the aim of this study was to evaluate the size and morphology of sella turcica in patients with type 1 diabetes compared with a healthy control group.
Methods
The study included 76 type 1 diabetic patients (38 boys, 38 girls; ages, 14.16 ± 2.46 years) and 76 controls (38 boys, 38 girls; ages, 14 ± 2.08 years). The groups were categorized as pubertal and postpubertal according to bone age. The length, height, and diameter of sella turcica were measured. Then the morphology of sella turcica was analyzed and categorized as normal, oblique anterior wall, bridging, double contour of the floor, irregularity in the posterior part of dorsum sellae, or pyramidal shape of the dorsum sellae. All measurements were made on tracings of cephalometric radiographs. Differences between the groups were tested with the Mann-Whitney U test. Categorical data were evaluated with the Fisher exact test, and the Bonferroni correction was made. The significance level was assigned as P <0.05.
Results
There was no statistically significant difference in the dimensions of sella between the diabetic patients (diameter, 12.20 ± 1.49 mm; length, 10.49 ± 1.55 mm; height, 8.07 ± 1.25 mm) and the controls (diameter, 12.45 ± 1.43 mm; length, 10.90 ± 1.73 mm; height, 8.29 ± 1.66 mm). However, diameter and length increased with age in the overall assessment. Length was greater in the postpubertal controls (11.39 ± 1.69 mm) compared with the pubertal controls (10.41 ± 1.64 mm). Diameter was greater in the postpubertal diabetic patients (1.283 ± 1.55 mm) than in the pubertal diabetic patients (11.56 ± 1.12 mm) and was specifically higher in postpubertal boys. Normal sella morphology was less common in general in the diabetic patients, particularly in the diabetic boys and diabetic pubertal boys ( P <0.05).
Conclusions
The measurements concerning sella were similar in the type 1 diabetic and control subjects, but dysmorphologic types were more common in diabetic patients.
Sella turcica is an important anatomic structure in the midcranial region that houses the pituitary gland; it was named according to its similar shape to Turkish saddles for the first time in Blancard’s Physical Dictionary (1693). The radiologic image of sella turcica on lateral cephalograms serves as a landmark to determine sella, the geometric center of this cavity, which is crucial for the cephalometric evaluations before, during, and after orthodontic therapy. For an orthodontist, lateral cephalograms are mostly to evaluate craniofacial anomalies, but they should also be seen as a tool that provides beneficial knowledge concerning cranial structures that can reflect signs of a genetic, congenital, or systemic disorder.
To date, because of its anatomic location, its relationship to the pituitary gland, and its developmental origin, the shape and dimensions of sella turcica and its possible connections to different craniofacial and endocrinologic pathologies had always been a hot spot for scientists. Previously published data showed that some diseases such as intrasellar adenomas, empty sella syndrome, Williams syndrome, Down syndrome, Axenfeld-Rieger syndrome with PITX2 mutation, lumbosacral myelomeningocele, and velocardiofacial syndrome caused changes in either dimensions or morphology of sella turcica.
The relationship between sella turcica morphology and different systemic disorders is mostly explained by the similarity of the developmental origins of sella and the mentioned disorders. Kjaer, Kjaer et al, and Kjaer and Niebuhr reported the difference in cell origins of the posterior and anterior walls of sella turcica. The anterior wall originates from neural crest cells, whereas the posterior wall originates from the notochord in the same way as the corpora of the vertebrae. Both walls are first formed as cartilage tissues; during the development process, they are differentiated to bone tissues. The morphology of sella turcica is similar before and after birth, but dimensions increase during growth and become stable around 15 years of age.
Type 1 diabetes, 1 of the 2 main types of diabetes, is a result of progressive pancreatic beta cell damage and ends with an absolute lack of insulin secretion. It is the most common chronic disease in children and adolescents, and there is an epidemic increase in newly diagnosed children each year. Detailed reports of the Epidemiology and Prevention of Diabetes study group showed that the incidence rate trends in type 1 diabetes across Europe continue to rise by approximately 3% to 4% every year, and relative increases were the highest in central and eastern European countries from 1989 through 2003.
According to the age at diagnosis, the numbers of new cases have peaks at 5 to 6 and 10 to 14 years of age. In general, more boys are diagnosed with type 1 diabetes than are girls, but how the sex difference affects how the disease arises is still unclear. The causes of the disease are associated with viral infections, other environmental factors, autoimmunity, and genetic mutations. Recent in-vitro studies have shown that neural crest cells, which are crucial for craniofacial development and formation of the anterior wall of sella turcica, promote survival and proliferation of beta cells and thus the secretion of insulin. As a chronic disease, type 1 diabetes adversely affects all organ systems in the body, especially the eyes, kidneys, reproductive organs, and bones.
Several diseases were investigated for a connection between them and the morphology of sella turcica regardless of their rare prevalence in adolescence. Despite its increasing incidence rate, effects on bone metabolism, possible genetic etiology, and relationship to neural crest cells, there is a lack of information in the literature about the interaction between type 1 diabetes and sella turcica morphology. Therefore, the aim of this study was to analyze the dimensions and morphology of sella turcica in patients with type 1 diabetes compared with healthy control subjects. It was hypothesized that the dimensions and morphology of sella turcica can be affected by type 1 diabetes, when compared with healthy control subjects.
Material and methods
The study consisted of lateral cephalograms of type 1 diabetic patients who were referred to Gazi University Department of Orthodontics, Faculty of Dentistry from the Department of Pediatric Endocrinology, Faculty of Medicine for dental consultation and evaluation of their craniofacial morphology. The number of patients that would give statistically relevant results in this cephalometric study was determined by a power analysis based on the study of El-Bialy et al. To test the difference between the groups with 90% accuracy, each subgroup needed 19 patients.
Approval for this study was obtained from the local ethical commission of Gazi University Faculty of Medicine, and informed consent forms prepared according to the Declaration of Helsinki were signed by every patient and his or her legal guardian for those under the age of 18 years.
From 552 patients, only 95 attended their appointments and agreed to take part in the project. A control group was randomly selected from patients seeking orthodontic treatment and matched with the diabetic group. The inclusion criteria for all participants are given in Table I in detail.
| Type 1 diabetes group |
|---|
| 10-18 years old |
| Treated with insulin and under control for 2 years or more |
| No other systemic diseases |
| No genetic or congenital craniofacial anomalies |
| Pubertal or postpubertal period according to hand-wrist radiographs |
| No previous orthodontic treatment |
| Control group |
|---|
| 10-18 years old |
| Skeletal Class I |
| Minimum crowding |
| Pubertal or postpubertal period according to hand-wrist radiographs |
| No systemic diseases |
| No genetic or congenital craniofacial anomalies |
| No previous orthodontic, prosthetic, or surgical treatment |
The effects of bone age and sex on the dimensions and morphology of sella turcica were also planned to be tested. Therefore, the study was composed of 152 lateral cephalograms (76 from diabetic patients, 76 from control subjects) that were equally distributed into subgroups according to bone age and sex. The assessments of bone age and remaining growth potential were made with hand-wrist radiographs according to the method of Greulich and Pyle. Patients with remaining growth potential more than 3% were included in pubertal group, whereas patients with growth potential less than 1% were categorized as the postpubertal group.
Patients with type 1 diabetes were under care in the pediatric endocrinology clinic for regulation of their blood glucose levels and observation of any complications of diabetes. The mean follow-up time of these patients was 5.23 ± 3.12 years. All diabetic patients were on insulin treatment, and the mean of their HbA1C levels, which indicated the blood glucose concentration in the past 3 months, was 8.23% ± 1.70%. The mean chronologic ages were 14.16 years (38 boys, 38 girls; age range, 10.08-17.6 years) for the diabetic group and 14 years (38 boys, 38 girls; age range, 10.3-17.8 years) for the control group. The mean chronologic ages of each subgroup are given in Table II .
| Puberty status | Sex | Chronologic age (y) | Bone age (y) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Control group | Pubertal | Male | 13.05 | 1.54 | 13.12 | 1.16 |
| Female | 11.86 | 0.88 | 12.25 | 0.76 | ||
| Total | 12.46 | 1.38 | 12.69 | 1.06 | ||
| Postpubertal | Male | 15.87 | 1.33 | 16.76 | 0.73 | |
| Female | 15.17 | 1.48 | 15.79 | 1.29 | ||
| Total | 15.52 | 1.44 | 16.28 | 1.15 | ||
| Total | Male | 14.46 | 2.02 | 14.94 | 2.08 | |
| Female | 13.51 | 2.06 | 14.02 | 2.08 | ||
| Total | 13.99 | 2.08 | 14.48 | 2.12 | ||
| Type 1 diabetes group | Pubertal | Male | 12.55 | 1.51 | 12.37 | 2.02 |
| Female | 11.89 | 1.86 | 12.01 | 2.14 | ||
| Total | 12.22 | 1.70 | 12.19 | 2.06 | ||
| Postpubertal | Male | 16.58 | 0.93 | 17.03 | 0.81 | |
| Female | 15.50 | 1.50 | 15.93 | 0.97 | ||
| Total | 16.04 | 1.34 | 16.48 | 1.04 | ||
| Total | Male | 14.56 | 2.39 | 14.70 | 2.81 | |
| Female | 13.70 | 2.47 | 13.97 | 2.58 | ||
| Total | 14.13 | 2.45 | 14.34 | 2.70 | ||
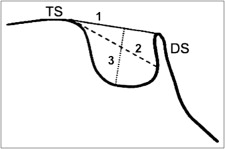
Lateral cephalograms for this study were taken with the Orthophos XG 5/Ceph (Sirona, Bensheim, Germany) at 73 KVp and 15 mA per second for 9.4 seconds. Evaluations were made in a blinded fashion. The second observer (M.D.) covered the names of the patients and their groups with a sticker to prevent any bias before the main observer (N.C.B.) assessed sella turcica. The radiographs were then manually traced with a 0.3-mm mechanical pencil, and measurements were made on the tracings by the main observer. The dimensions of sella turcica—length, diameter, and height ( Fig 1 )—were measured according to the definitions of Silverman. Length is the anteroposterior distance between the crest of tuberculum sella and dorsum sella, diameter is the anteroposterior distance between the crest of tuberculum sella and the deepest point in the posterior wall of sella turcica, and height is the perpendicular distance from the line drawn between tuberculum sella and dorsum sella (length) to the floor of sella. Sella turcica morphology was grouped according to the definitions of Axelsson et al : normal, oblique anterior wall, double contour of the floor, bridging, irregularity or notching in the posterior part of dorsum sella, pyramidal shape of dorsum sella, and a combination of more than 1 irregularity.
Statistical analysis
Data were analyzed using SPSS software for Windows (version 16.0; SPSS, Chicago, Ill). The normality of the data was checked with Kolmogorov-Smirnov (n >50) and Shapiro-Wilks (n >50) tests. Because the data were not distributed normally, nonparametric tests were preferred. Differences between groups were tested with the Mann-Whitney U test, and categorical data were evaluated by the Fisher exact test; the Bonferroni correction was made. The level of significance was established as P <0.05.
To define the intraobserver error rate, 60 lateral cephalograms (30 from diabetic patients, 30 from controls) were randomly selected, and linear measurements and categorizations of sella turcica were repeated 1 month after the initial tracings. The reproducibility and the strength of the measurements were evaluated by the intraclass correlation coefficient. A coefficient of repeatability for linear measurements was derived according to the Bland-Altman method, which was equal to 2 SD of the differences between the first and repeated measurements. A precision value was calculated by dividing the coefficient of repeatability by the mean of the first and second measurements. Precision values smaller than 10% were regarded as measurements in agreement and acceptable for reproducibility. For all variables, the intraclass correlation coefficients were between 0.91 and 1.00. Precision values for the linear measurements were between 2.35% and 4.29%, which all showed good reproducibility of the first measurements.
Results
For both groups, the chronologic and bone ages of the subjects were correlated to each other, and no statistically significant difference was found between the mean values of the groups ( P >0.05) ( Table II ).
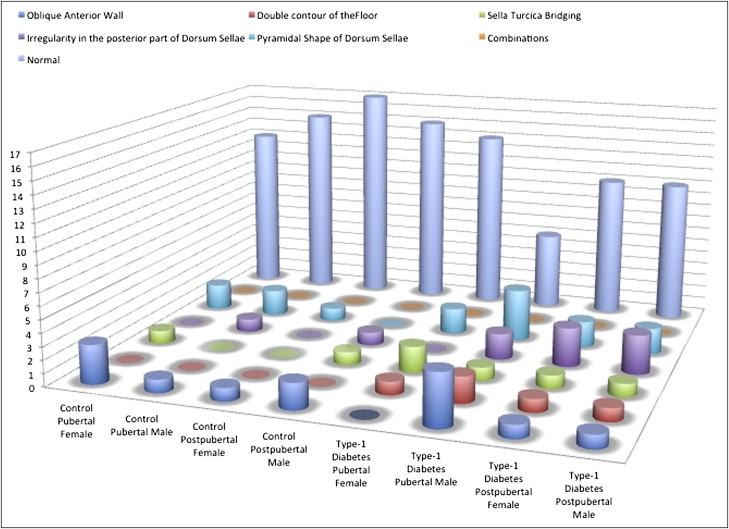
The general distribution of morphologic diversions of sella turcica in the diabetic patients and the control group is given in Figure 2 and Table III . Since no subject represented a combination in any group, this classification was omitted from Table III .
Intragroup comparisons showed no statistically significant differences in the sexes between the pubertal and postpubertal subgroups for both the diabetic and control groups.
Among the general study population, in the diabetic group, a normal sella turcica was less common (diabetic, 55.3%; control, 78.9%) ( P <0.05), but no other morphologic variation was significantly more frequent when compared with the control group.
No statistical difference was detected between the girls, but the percentage of boys with a normal sella turcica in the diabetic group (44.7%) was significantly lower than in the control group (78.9%) ( P <0.05). When the effect of the interaction between type 1 diabetes, bone age, and sex on the morphology of sella turcica was evaluated, the percentage of pubertal boys with a normal sella turcica in the diabetic group (31.6%) was significantly lower than in the control group (78.9%) ( P <0.05).
In the diabetic group, the length and the diameter of sella were significantly smaller in the pubertal group compared with the postpubertal subjects ( P <0.05 and P <0.001, respectively). However, there was no significant difference between these 2 groups for the height of sella ( P >0.05).
In the control group, only length differed significantly between the pubertal and postpubertal groups; it was longer in the postpubertal group ( P <0.01), and there were no statistically significant differences concerning depth and height ( P >0.05).
Intergroup comparisons showed that the diameter of sella was smaller in the diabetic pubertal group than in the control pubertal group, and in the diabetic pubertal girls than in the control pubertal girls ( P <0.05). The height of sella was smaller in the diabetic pubertal, the diabetic female, and the diabetic postpubertal female groups compared with the control pubertal, the control female, and the control postpubertal female groups, respectively. The comparisons of the groups according to bone age, sex, and their interactions are given in Tables IV through VI .
| Pubertal (n = 38) | Postpubertal (n = 38) | P | Pubertal girls (n = 19) | Postpubertal girls (n = 19) | P | Pubertal boys (n = 19) | Postpubertal boys (n = 19) | P | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||
| T1DM | |||||||||||||||
| Diameter | 11.57 | 1.13 | 12.78 | 1.44 | <0.001 ‡ | 11.55 | 0.90 | 12.55 | 1.34 | 0.013 ∗ | 11.58 | 1.35 | 13.00 | 1.53 | 0.004 † |
| Length | 10.09 | 1.41 | 10.89 | 1.59 | 0.023 ∗ | 10.29 | 1.19 | 10.79 | 1.69 | 0.298 | 9.89 | 1.60 | 11.00 | 1.53 | 0.036 ∗ |
| Height | 7.80 | 1.06 | 8.34 | 1.37 | 0.085 | 7.74 | 0.86 | 7.92 | 1.20 | 0.729 | 7.87 | 1.25 | 8.76 | 1.43 | 0.053 |
| Control | |||||||||||||||
| Diameter | 12.16 | 1.35 | 12.67 | 1.25 | 0.109 | 12.47 | 1.26 | 12.68 | 1.11 | 0.773 | 11.84 | 1.38 | 12.66 | 1.41 | 0.081 |
| Length | 10.41 | 1.64 | 11.34 | 1.63 | 0.007 † | 10.55 | 1.44 | 11.05 | 1.27 | 0.179 | 10.26 | 1.85 | 11.63 | 1.92 | 0.022 ∗ |
| Height | 8.41 | 1.28 | 8.41 | 1.44 | 0.97 | 8.53 | 1.35 | 8.58 | 1.67 | 0.908 | 8.29 | 1.24 | 8.24 | 1.18 | 0.908 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


