Introduction
The purpose of this 2-arm parallel study was to evaluate the dentoskeletal effects of rapid maxillary expansion with differential opening (EDO) compared with the hyrax expander in patients with complete bilateral cleft lip and palate.
Methods
A sample of patients with complete bilateral cleft lip and palate was prospectively and consecutively recruited. Eligibility criteria included participants in the mixed dentition with lip and palate repair performed during early childhood and maxillary arch constriction with a need for maxillary expansion before the alveolar bone graft procedure. The participants were consecutively divided into 2 study groups. The experimental and control groups comprised patients treated with rapid maxillary expansion using EDO and the hyrax expander, respectively. Cone-beam computed tomography examinations and digital dental models of the maxillary dental arches were obtained before expansion and 6 months postexpansion. Standardized cone-beam computed tomography coronal sections were used for measuring maxillary transverse dimensions and posterior tooth inclinations. Digital dental models were used for assessing maxillary dental arch widths, arch perimeters, arch lengths, palatal depths, and posterior tooth inclinations. Blinding was used only during outcome assessment. The chi-square test was used to compare the sex ratios between groups ( P <0.05). Intergroup comparisons were performed using independent t tests with the Bonferroni correction for multiple tests.
Results
Fifty patients were recruited and analyzed in their respective groups. The experimental group comprised 25 patients (mean age, 8.8 years), and the control group comprised 25 patients (mean age, 8.6 years). No intergroup significant differences were found for age, sex ratio, and dentoskeletal variables before expansion. No significant differences were found between the EDO and the hyrax expander groups regarding skeletal changes. The EDO promoted significantly greater increases of intercanine width (difference, 3.63 mm) and smaller increases in canine buccal tipping than the conventional hyrax expander. No serious harm was observed other than transitory variable pressure sensations on the maxillary alveolar process in both groups.
Conclusions
The EDO produced skeletal changes similar to the conventional hyrax expander. The differential expander is an adequate alternative to conventional rapid maxillary expanders when there is need for greater expansion in the maxillary dental arch anterior region.
Registration
This trial was not registered.
Protocol
The protocol was not published before trial commencement.
Funding
This study received financial support from FAPESP (process number 2009/17622-9). As a possible conflict of interest, a patent with an EDO was submitted in March 2011 to the National Institute of Industry Property and is still in process. However, we believe that this is a natural step of translational research (bench-to-bedside), and we guarantee that the scientific results are true.
Highlights
- •
Rapid maxillary expansion with differential opening (EDO) is an innovation for improving orthodontic care of patients with complete bilateral cleft lip and palate (BCLP).
- •
The dentoskeletal effect of EDO was compared with that with a hyrax expander in patients with BCLP.
- •
EDO caused greater increase of the intercanine width compared with a hyrax expander.
Maxillary arch constriction is a frequent clinical feature in patients with complete bilateral cleft lip and palate (BCLP). Both the absence of the midpalatal bone and the soft tissue traction produced by lip and palate repair promote arch constriction. Although the transversal deficiency may occur in all regions of the maxillary dental arch, it is more pronounced in the canine region. Previous studies analyzing the maxillary arch form in patients with BCLP have demonstrated that the maxillary segments move and rotate toward the medial aspect with the fulcrum located in the maxillary tuberosity, determining an anteriorly progressive constriction. Thus, the intercanine distance shows a greater reduction compared with the intermolar width in these patients.
Rapid maxillary expansion (RME) is an orthopedic procedure that aims to correct the maxillary arch constriction by transversal separation of the maxillary halves. Especially in patients with cleft lip and palate, RME can be performed in the late mixed dentition before the secondary alveolar bone graft procedure. The aim of the maxillary expansion is not only to treat the posterior crossbite, but also to align the maxillary segments. This procedure increases the alveolar cleft width and creates room for bone graft placement. Additionally, it facilitates the transoperative procedures for nasal mucosa suture before the filling of the alveolar cleft with bone graft. For these reasons, the correction of the maxillary arch constriction by maxillary expansion is necessary in most patients with BCLP.
Currently, the appliances for RME may produce either a conventional or a fan-type expansion. Conventional expansion produces similar transversal increases in the anterior and posterior regions of the maxillary dental arch. On the other hand, fan-type expanders promote a transversal increase only in the anterior region of the dental arch. Recently, a novel maxillary expander was designed especially for achieving different amounts of expansion in the anterior and posterior regions of the maxillary dental arch in patients with complete BCLP.
Specific objectives or hypotheses
The purpose of this study was to evaluate the dentoskeletal effects of the expander with differential opening (EDO) in comparison with the conventional hyrax expander. The hypothesis was that the EDO and the hyrax expander have similar effects.
Material and methods
Trial design and any changes after trial commencement
This study was a nonrandomized controlled clinical trial, in which the participants of each group were prospectively recruited and consecutively divided into 2 study groups. No changes in methods occurred after trial commencement.
Participants, eligibility criteria, and settings
A sample of orthodontic patients with complete BCLP was recruited prospectively from August 2010 to June 2014, in the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo, in Bauru, Brazil. Inclusion criteria were patients in the mixed dentition with lip and palate repair performed during early childhood and maxillary arch constriction with a need for maxillary expansion before the alveolar bone graft procedure. Exclusion criteria were syndromes, previous orthodontic treatment, and periodontal disease.
This study was approved by the research institutional board of the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (protocol number 60/2010), before trial commencement. Parents signed the informed consent form before intervention if the patients were minors.
Interventions
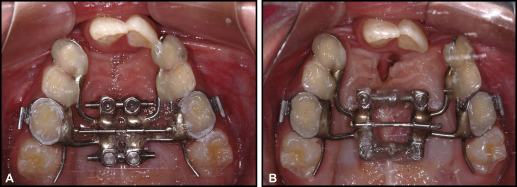
The participants were consecutively divided into 2 groups. The experimental group was recruited from August 2010 to July 2012 and comprised patients treated with the EDO ( Fig 1 , A ). Because the participants were in the mixed dentition, appliance anchorage was provided by bands adapted on either the maxillary permanent first molars or the deciduous second molars, and circumferential clamps were bonded to the maxillary deciduous canines. When the maxillary deciduous second molars were banded, a lingual extension wire was placed in the partially erupted maxillary permanent first molars. Both anterior and posterior screws were activated with a complete turn a day (approximately 0.8 mm) until achieving an overcorrection at the molar region, with the palatal cusp tip of the maxillary posterior teeth contacting the buccal cusp tip of the mandibular posterior teeth. During the following days, only the anterior screw was activated until achieving a slight overcorrection of 2 mm in the intercanine distance. The amount of expansion was determined individually, depending on the severity of the maxillary arch constriction. Mean activations were 5 mm (SD, 1.77) and 7 mm (SD, 1.99) with the posterior and anterior screws, respectively. After the active period of RME, the screws were fixed with acrylic resin, and the appliances were kept as retainer for 6 months ( Fig 1 , B ).
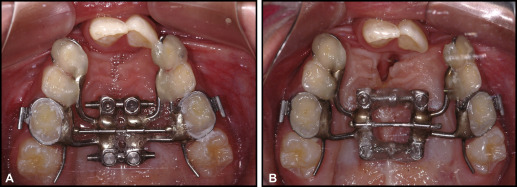
The control group was recruited from August 2012 to June 2014 and comprised patients treated with a conventional hyrax expander. Bands were adapted on either the maxillary permanent first molars or the deciduous second molars, and circumferential clamps were bonded to the maxillary deciduous canines. Similarly to the experimental group, a lingual extension wire was placed on the partially erupted maxillary permanent first molars when the maxillary deciduous second molars were banded. The expander screw (Dentaurum, Ispringen, Germany) was activated with a complete turn a day (approximately 0.8 mm) until achieving an overcorrection in the molar region where the palatal cusp tip of the maxillary posterior teeth contacted the buccal cusp tip of the mandibular posterior teeth. The mean expansion amount was 5 mm (SD, 2.79). After the expansion active phase, the screw was fixed with acrylic resin, and the appliances were kept in the dental arch as retainers for 6 months.
Cone beam computed tomography (CBCT) and dental models of the maxillary arch were obtained before expansion and 6 months postexpansion, after appliance removal.
CBCT examinations were performed using the i-CAT New Generation System (Imaging Sciences International, Hatfield, Pa). The technical parameters for image acquisition were 120 kVp, 8 mA, 26.9 seconds, field of view of 13 cm, and voxel size of 0.25 mm. CBCT examinations replaced conventional radiographs for orthodontic treatment planning, before expansion and for bone graft planning after expansion.
CBCT images were measured by 1 examiner (R.C.M.C.L.) using the Nemoscan software (Nemotec, Madrid, Spain). Before measurement, the head image position was standardized with the Frankfort plane and the infraorbital line parallel to the horizontal plane in the lateral and frontal views, respectively. In the axial plane, the ethmoidal septum was positioned in the vertical plane.
The dental models were digitized using a scanner (R700 3D; 3Shape, Copenhagen, Denmark). OrthoAnalyzer 3D software (3Shape) was used by 1 examiner (L.R.C.) to measure the complementary primary outcomes.
Outcomes (primary and secondary) and any changes after trial commencement
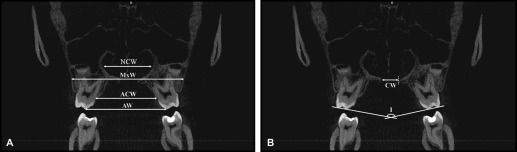
CBCT primary outcomes were maxillary transverse dimensions and posterior tooth inclinations. Transverse dimensions of the maxilla were measured in 2 coronal images perpendicular to the midsagittal plane, one passing through the center of the palatal root of the maxillary right permanent first molar (molar region), and other displaced 15 mm anteriorly (premolar region). Figure 2 illustrates the linear variables obtained in the coronal images before and after expansion. Posterior tooth inclination was measured only in the molar coronal image ( Fig 2 , B ).
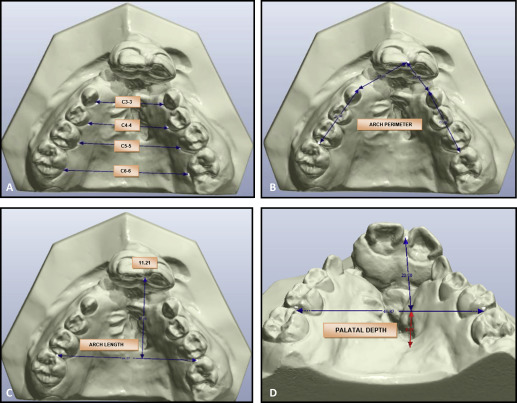
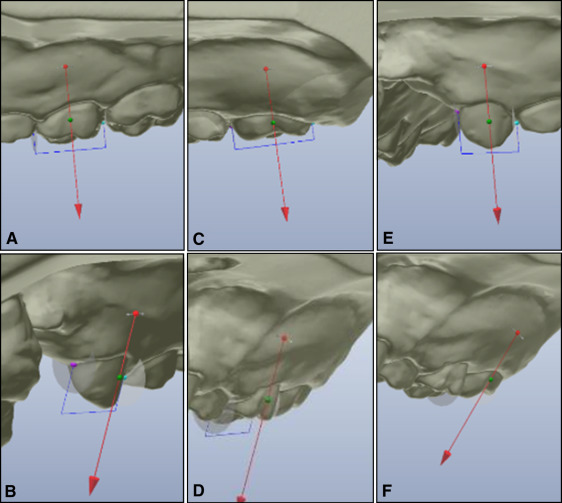
Digital dental model primary outcomes included maxillary dental arch widths (at the deciduous canines, first molars or permanent first premolars, second molars or permanent second premolars, and permanent first molars), arch perimeters, arch lengths, palatal depths, and inclinations of the deciduous canines, deciduous second molars, and permanent first molars ( Figs 3 and 4 ).
Sample size calculation
Calculation of the sample size was based on the ability to detect a difference in maxillary width of 1.0 mm (SD, 1.10), with an alpha error of 5% and a test power of 80%. Twenty participants were required in each group.
Interim analyses and stopping guidelines
Not applicable.
Randomization
Randomization was not performed in this study. Patients were treated consecutively starting with the experimental group.
Blinding
Blinding of both patient and operator was not possible in this study. However, the outcome assessment was blinded.
Statistical analyses
All measurements were made twice by the same examiner with a month interval. Statistical analysis was performed, taking into account the means of the 2 measurements. The mean and standard deviation of each variable were calculated before and after expansion, as well as the changes between these stages. The Shapiro-Wilk normality test, followed by the Levene test for equality of variances, showed a normal distribution of the variables, and parametric tests were used.
Random and systematic errors were calculated by comparing the first and second measurements with the Bland-Altman analysis and the intraclass coefficient correlation.
Chi-square and independent t tests were respectively used to compare sex ratios and initial ages between groups ( P <0.05). Intergroup comparisons were performed using independent t tests with the Bonferroni correction for multiple tests ( t tests on a set of 9 CBCT measurements and 10 digital dental model measurements). Associated 95% confidence intervals (CIs) were calculated.
Multiple linear regression analysis was used to verify whether banded molars were a confounding factor for inclination changes.
Material and methods
Trial design and any changes after trial commencement
This study was a nonrandomized controlled clinical trial, in which the participants of each group were prospectively recruited and consecutively divided into 2 study groups. No changes in methods occurred after trial commencement.
Participants, eligibility criteria, and settings
A sample of orthodontic patients with complete BCLP was recruited prospectively from August 2010 to June 2014, in the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo, in Bauru, Brazil. Inclusion criteria were patients in the mixed dentition with lip and palate repair performed during early childhood and maxillary arch constriction with a need for maxillary expansion before the alveolar bone graft procedure. Exclusion criteria were syndromes, previous orthodontic treatment, and periodontal disease.
This study was approved by the research institutional board of the Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo (protocol number 60/2010), before trial commencement. Parents signed the informed consent form before intervention if the patients were minors.
Interventions
The participants were consecutively divided into 2 groups. The experimental group was recruited from August 2010 to July 2012 and comprised patients treated with the EDO ( Fig 1 , A ). Because the participants were in the mixed dentition, appliance anchorage was provided by bands adapted on either the maxillary permanent first molars or the deciduous second molars, and circumferential clamps were bonded to the maxillary deciduous canines. When the maxillary deciduous second molars were banded, a lingual extension wire was placed in the partially erupted maxillary permanent first molars. Both anterior and posterior screws were activated with a complete turn a day (approximately 0.8 mm) until achieving an overcorrection at the molar region, with the palatal cusp tip of the maxillary posterior teeth contacting the buccal cusp tip of the mandibular posterior teeth. During the following days, only the anterior screw was activated until achieving a slight overcorrection of 2 mm in the intercanine distance. The amount of expansion was determined individually, depending on the severity of the maxillary arch constriction. Mean activations were 5 mm (SD, 1.77) and 7 mm (SD, 1.99) with the posterior and anterior screws, respectively. After the active period of RME, the screws were fixed with acrylic resin, and the appliances were kept as retainer for 6 months ( Fig 1 , B ).
The control group was recruited from August 2012 to June 2014 and comprised patients treated with a conventional hyrax expander. Bands were adapted on either the maxillary permanent first molars or the deciduous second molars, and circumferential clamps were bonded to the maxillary deciduous canines. Similarly to the experimental group, a lingual extension wire was placed on the partially erupted maxillary permanent first molars when the maxillary deciduous second molars were banded. The expander screw (Dentaurum, Ispringen, Germany) was activated with a complete turn a day (approximately 0.8 mm) until achieving an overcorrection in the molar region where the palatal cusp tip of the maxillary posterior teeth contacted the buccal cusp tip of the mandibular posterior teeth. The mean expansion amount was 5 mm (SD, 2.79). After the expansion active phase, the screw was fixed with acrylic resin, and the appliances were kept in the dental arch as retainers for 6 months.
Cone beam computed tomography (CBCT) and dental models of the maxillary arch were obtained before expansion and 6 months postexpansion, after appliance removal.
CBCT examinations were performed using the i-CAT New Generation System (Imaging Sciences International, Hatfield, Pa). The technical parameters for image acquisition were 120 kVp, 8 mA, 26.9 seconds, field of view of 13 cm, and voxel size of 0.25 mm. CBCT examinations replaced conventional radiographs for orthodontic treatment planning, before expansion and for bone graft planning after expansion.
CBCT images were measured by 1 examiner (R.C.M.C.L.) using the Nemoscan software (Nemotec, Madrid, Spain). Before measurement, the head image position was standardized with the Frankfort plane and the infraorbital line parallel to the horizontal plane in the lateral and frontal views, respectively. In the axial plane, the ethmoidal septum was positioned in the vertical plane.
The dental models were digitized using a scanner (R700 3D; 3Shape, Copenhagen, Denmark). OrthoAnalyzer 3D software (3Shape) was used by 1 examiner (L.R.C.) to measure the complementary primary outcomes.
Outcomes (primary and secondary) and any changes after trial commencement
CBCT primary outcomes were maxillary transverse dimensions and posterior tooth inclinations. Transverse dimensions of the maxilla were measured in 2 coronal images perpendicular to the midsagittal plane, one passing through the center of the palatal root of the maxillary right permanent first molar (molar region), and other displaced 15 mm anteriorly (premolar region). Figure 2 illustrates the linear variables obtained in the coronal images before and after expansion. Posterior tooth inclination was measured only in the molar coronal image ( Fig 2 , B ).


