FIGURE 14-1An American Dental Association dental claim form. A, Front. B, Back (Courtesy American Dental Association, Chicago.)
Most dental offices use computerized practice management software that generates and prints claim forms in a standard, ADA-compliant format. If the office does not use computers or the carrier requires the use of a specific form, the administrative assistant can legibly print or type the required information on the claim form. The assistant must review the paper claims, attach any required radiographs, and add documentation where needed. Claims are batched by carrier and then mailed out.
Note: When radiographs are mailed, they must be placed in a container, such a mount or an envelope. The patient’s name, the dental office’s name and address, and the tooth number or the area of the mouth shown on the film must be clearly written on the container. Carriers are not required to return radiographs, so any sent with a claim should be duplicates, and the original should be retained in the patient’s records.
Electronic Claim Form
Nearly all dental offices have replaced the pegboard and appointment book with computers and sophisticated practice management software. The percentage of dental offices submitting all or part of their claims electronically continues to rise. Some carriers report that they receive more than 70% of dental claims electronically. As compared with the time and expense of preparing and mailing paper claims, electronic claims submission can be faster, less expensive, and more accurate. E-claims can be submitted through a clearinghouse or directly to the carrier through a web-based portal.
Offices that file e-claims must comply with federal laws governing electronic transactions that include personal health information (PHI). Under the Health Insurance Portability and Accountability Act of 1996 (HIPAA), all healthcare providers, health plans, and healthcare clearinghouses that transmit PHI electronically must use a universal language, a standard format, and a government-assigned unique identification number. HIPAA also mandates security and privacy standards for electronic transactions, as discussed in Chapter 7.
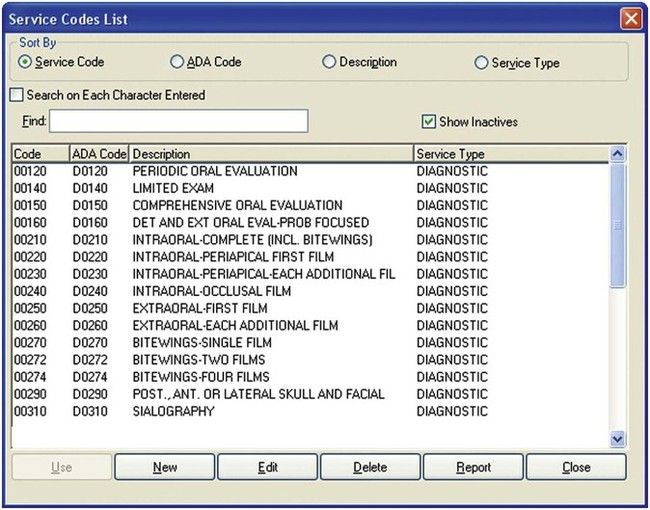
• The Code: The universal language used for electronic transmission of dental data is the ADA Code on Dental Procedures and Nomenclature (also known as the Code), which is updated every 2 years (Figure 14-2). Current Dental Terminology (CDT) manuals, which are the only official sources for the Code, can be purchased from the ADA; these list the procedure codes with nomenclature and descriptors, changes from the previous code, and other helpful information (Figure 14-3).
FIGURE 14-2Pull-down screen of American Dental Association service codes. (Courtesy Patterson Dental, St. Paul, Minnesota.)
FIGURE 14-3Current Dental Terminology (CDT), the only official source for dental service codes, is published by the American Dental Association and updated every 2 years. (Courtesy American Dental Association, Chicago, Illinois.)
• Electronic data formats: HIPAA mandates the use of standardized formats for electronic transactions of health information. The standard formats are used for claims, remittance advice (explanation of benefits), eligibility inquiry and response, prior authorization and referral, and claims status inquiry and response. Attachments to the claim form (e.g., radiographs) can also be submitted electronically with the use of specialized software or services that assign a tracking number to match the supporting documentation of the claim. Most carriers prefer digital radiographs because they are easier and more cost-effective to handle and because the possibility of films becoming detached or lost is decreased.
• Unique identifiers: Dental offices that submit claims or claims attachments electronically or that use the Internet to look up eligibility, benefits, or claims status are required to have and use a National Provider Identifier (NPI). The NPI is a unique and permanent 10-digit number that identifies the dentist or practice and that replaces any other identifiers used in electronic transactions. (It does not replace the tax identification number [TIN] or the treating dentist’s state license number, because these are used for purposes other than identification.) To get an NPI, a dentist or a dental practice applies to an agency designated by the federal government.
Via Clearinghouse
A clearinghouse is a company that accepts the transmission of raw data, scans it for errors or missing information, and then transforms it into the appropriate data format for submission to the benefits carrier. The clearinghouse charges either a set amount per claim or a monthly fee for this service.
With the use of practice management software, the dental office administrative assistant collects the patient and treatment information that is ready to be billed to a benefits carrier and transmits it to the clearinghouse. The clearinghouse reformats the data and then transmits any claims with missing or incomplete information back to the dental office for correction. The formatted claims are sorted by benefits carrier or insurance company and mass-transmitted to the carrier for processing. The clearinghouse can also print and mail paper claim forms to the few carriers that are unable to accept electronic claims.
Direct to Carrier
The dental office has to be computerized and connected to the Internet to transmit claims directly to benefits carriers. Most major carriers provide this service free of charge. To submit, the administrative assistant goes online to the carrier’s website or portal and enters claim information into an electronic claim form, which can begin processing immediately. Entering claims via the portal eliminates the sorting, scanning, and data entry that a carrier must do with paper claims, so processing time is reduced by an average of 2 to 4 days. In most cases, routine claims are adjudicated and released for payment within 24 hours of entering the carrier’s system. The dental practice’s transaction history—including payments, rejections, and predeterminations—is maintained in a highly secure system; it can be accessed or downloaded only with the use of the dentist’s unique password.
Code on Dental Procedures and Nomenclature
The ADA Code on Dental Procedures and Nomenclature (commonly known as the Code) is used to report dental services and procedures to dental benefits plans. Per HIPAA, the ADA updates the Code every other year (in odd-numbered years) and publishes the Code in a reference manual called Current Dental Terminology (CDT). These procedure codes identify and describe each specific dental treatment. The codes and the dentist’s fees are used to report and bill treatment to the benefits carrier. Each procedure code starts with a “D” followed by four numerals. The codes are categorized according to different types of treatment:
Diagnostic
D0100 through D0999
Preventive
D1000 through D1999
Restorative
D2000 through D2999
Endodontics
D3000 through D3999
Periodontics
D4000 through D4999
Prosthetics, removable
D5000 through D5899
Maxillofacial prosthetics
D5900 through D5999
Implant services
D6000 through D6199
Prosthodontics, fixed
D6200 through D6999
Oral and maxillofacial surgery
D7000 through D7999
Orthodontics
D8000 through D8999
Adjunctive general services
D9000 through D9999
Coordination of Benefits
Coordination of benefits (COB) is the procedure used to determine the order of liability when a person is covered by more than one plan. Dental benefits carriers follow rules established by state law to determine which plan pays first (primary carrier) and the financial obligation of any additional carrier (e.g., secondary, tertiary). The objective is to provide the maximum allowable benefit (MAB) without exceeding the actual fee charged.
Determining the Order of Liability
To identify the primary plan, the administrative assistant needs to know whether the patient is the subscriber or a dependent and whether there are any special COB rules for either plan. The primary carrier must meet at least one of the following criteria:
• A plan has a no-COB clause. If the plan does not coordinate benefits, it is the primary plan.
• The patient is the employee (subscriber). The plan that covers the patient as an active employee (subscriber) is always primary over a plan that covers the person as a retiree, spouse, dependent, or COBRA-qualified beneficiary. If the patient is the subscriber for both plans, the plan that covers the person as an active employee is primary. If the subscriber is an active employee under both plans, then the plan that has covered the individual the longest is primary.
• The patient is a dependent child. Most carriers follow the birthday rule: the plan of the parent whose birthday comes first in a calendar year is primary for the children. For example, if the mother’s birthday is in January and the father’s birthday is in March, then the mother’s plan is primary for all of the children. Some carriers may have a different coordination rule, such as the gender rule, in which the father’s plan is always primary.
• The patient is a dependent child of divorced or legally separated parents. If a court decree makes one parent responsible for healthcare expenses, then that parent’s plan is primary. If a court decree does not mention healthcare, default rules for determining the order of liability are as follows:
•Natural parent with custody
•Spouse of natural parent with custody
•Natural parent without custody
Only gold members can continue reading. Log In or Register to continue