History of the Procedure
Early attempts of vascularized iliac crest harvest were based on the superficial iliac vessels supplying the groin. Success rates were limited before surgeons gained an accurate understanding of the blood supply to the ilium. In 1979, Taylor and Sanders recognized the superiority of the deep circumflex iliac artery (DCIA) as the dominant blood supply to the bone. Only a year later, reports of mandible reconstruction emerged using this new flap. Surgeons quickly realized that the skin paddle associated with this flap was bulky and often required secondary revision procedures when placed in the oral cavity. The internal oblique free muscle flap, based on the ascending branch of the DCIA, was first described in 1984 for lower extremity reconstruction. This muscle quickly began to replace the skin paddle as the soft tissue component of choice when harvesting the DCIA free flap. In 1989, Urken and colleagues described the iliac crest bone flap with the internal oblique muscle to resurface oral and pharyngeal defects when combined with mandible reconstruction. The DCIA flap with internal oblique was eventually used for maxillary reconstruction as popularized by Brown almost a decade later. Further refinements of the internal oblique muscle technique were soon published.
History of the Procedure
Early attempts of vascularized iliac crest harvest were based on the superficial iliac vessels supplying the groin. Success rates were limited before surgeons gained an accurate understanding of the blood supply to the ilium. In 1979, Taylor and Sanders recognized the superiority of the deep circumflex iliac artery (DCIA) as the dominant blood supply to the bone. Only a year later, reports of mandible reconstruction emerged using this new flap. Surgeons quickly realized that the skin paddle associated with this flap was bulky and often required secondary revision procedures when placed in the oral cavity. The internal oblique free muscle flap, based on the ascending branch of the DCIA, was first described in 1984 for lower extremity reconstruction. This muscle quickly began to replace the skin paddle as the soft tissue component of choice when harvesting the DCIA free flap. In 1989, Urken and colleagues described the iliac crest bone flap with the internal oblique muscle to resurface oral and pharyngeal defects when combined with mandible reconstruction. The DCIA flap with internal oblique was eventually used for maxillary reconstruction as popularized by Brown almost a decade later. Further refinements of the internal oblique muscle technique were soon published.
Indications for the Use of the Procedure
The DCIA free flap is an excellent source of bone and soft tissue for composite defects of the head and neck. Of the major sources of vascularized bone, the iliac crest provides the most anatomic reconstruction of the mandible due to the natural contours corresponding to the curvature of the mandible. In addition, no other vascularized bone source can replace both the height and width of the native mandible. This large quantity of available bone makes the DCIA free flap especially appealing when planning for osseointegrated dental implant placement.
For intraoral reconstruction, the internal oblique muscle is often used as the soft tissue component to avoid the unnecessary bulk of the cutaneous skin paddle. This muscle layer drapes easily in the oral cavity and can be trimmed as needed. Within a month the muscle is mucosalized and conforms nicely to the contours of the bone. Although the skin paddle is notoriously bulky, perforator dissection techniques have been described, which allow thinning and customization of the skin paddle. However, the skin perforator may be unreliable and should be confirmed to be present preoperatively. For through-and-through defects of the oral cavity requiring both mucosal and skin replacement, the internal oblique may be used to resurface the oral cavity, while a cutaneous skin paddle simultaneously replaces the external skin defect.
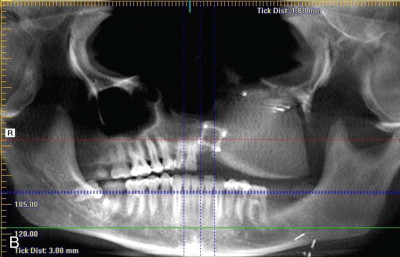
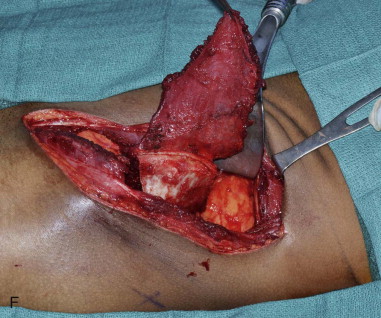
For maxillary reconstruction, the iliac crest may be positioned vertically ( Figure 118-1 ) or horizontally as dictated by the defect. The internal oblique muscle is draped across the palate to separate the sinonasal cavity from the oral cavity. This muscle eventually atrophies and becomes a taut band of vascularized tissue resembling the native hard palate.

Limitations and Contraindications
Although the DCIA free flap has great versatility, certain disadvantages exist. The skin paddle has limited mobility in relation to the bone, making accurate reconstruction of complex defects more challenging. Superior chimeric properties exist within the subscapular system, which allows for easier three-dimensional insetting. The bone stock of the vascularized iliac crest is generally limited to 16 cm, which is not sufficient for total mandibular reconstruction. Osteotomies must be performed on the lateral surface of the ilium to protect the vascular supply on the medial surface. This produces open segments at the osteotomy sites, which may need to be grafted with corticocancellous bone. Lastly, the vascular pedicle is relatively short. With an average pedicle length of 5 to 7 cm, vein grafting should be anticipated in vessel-depleted necks or with maxillary reconstruction.
Contraindications to harvest of the DCIA free flap include prior surgery in the region of the flap harvest, existing hernias, and obesity. Preoperative physical exam should focus on the presence of scars or hernias. Obesity is a relative contraindication, as the bulky skin paddle is less reliable and often too large to be useful.
Technique: DCIA with Internal Oblique Muscle
Step 1:
Positioning and Skin Marking
The patient is placed supine with the iliac crest exposed. Draping should include the midline of the abdomen medially, the costal margin superiorly, the groin crease inferiorly, and down to the operating room bed laterally. For larger bone flaps, a cushioned beanbag under the hip provides additional exposure to the gluteal region. The anterior superior iliac spine is palpated and marked along with the remainder of the iliac crest posteriorly. An incision line is drawn along the superior aspect of the iliac crest. The incision extends from the palpable femoral pulse in the groin crease to the midaxillary line posteriorly ( Figure 118-2, A ).





Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


