Introduction
Cortical bone thickness and bone depth are important factors when placing an orthodontic mini-implant. The objective of this study was to investigate both variables for the palatal alveolar process.
Methods
Thirty dry human skulls were imaged by using cone-beam computed tomography technology. Two-dimensional slices bisecting the posterior interdental sites were generated, and cortical bone thickness and bone depth were measured at 4, 8, and 12 mm from the alveolar crest. Two-way repeated measures analysis of variance (ANOVA) was used to analyze the measurements.
Results
Interdental site and measurement level had a significant impact on both cortical bone thickness and bone depth. Cortical bone thickness was typically greatest at the 8-mm measurement level and more anterior interdental sites. Bone depth decreased with higher measurement levels and was smallest at the most posterior-superior measurement points.
Conclusions
Cortical bone thickness and bone depth of the palatal alveolar process are, on average, favorable for the insertion of orthodontic mini-implants; however, some sites should routinely be avoided to prevent damage to the maxillary sinus unless 3-dimensional imaging is available.
It is generally accepted that anatomic factors should be included in the planning for an orthodontic mini-implant (OMI). Multiple anatomic factors are important for the long-term success of an OMI ( Table I ). Of those, the group of osseous factors is of particular interest, since it is the bone that ultimately is responsible for the anchorage capacity of the OMI. It appears that the majority of anchorage capacity results from the quality and quantity of cortical bone, whereas cancellous bone probably contributes little to the stability of OMIs.
| Osseous factors | Soft-tissue factors | Vulnerable structures |
|---|---|---|
| Cortical bone thickness | Quality (mucosa vs attached gingiva) | Roots |
| Bone depth | Tissue thickness | Nerves |
| Bone mineral density | Mobility | Blood vessels |
| Tension (frenum proximity) | Sinus/nasal cavity |
Another important factor to determine the suitability of a potential insertion site is overall bone availability or bone depth. There should be enough bone to place an OMI of a certain length without contralateral perforation or perforation into the maxillary sinus or the nasal cavity, thus creating an oral-antral connection.
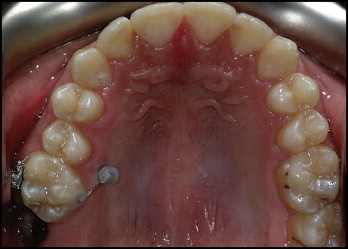
Because of their importance, cortical bone thickness and bone depth have been investigated thoroughly for most OMI insertion sites. However, to date, no comprehensive data exist for a clinically very useful site: the palatal aspect of the posterior alveolar process ( Fig 1 ).
The purpose of this study was therefore to investigate cortical bone thickness and bone depth of the posterior palatal alveolar process.
Material and methods
The sample consisted of 30 dry skulls of white adults from the Hamman-Todd Osteological Collection at the Cleveland Museum of Natural History, Cleveland, Ohio (26 male, 4 female; average age, 31.2 ± 10.6 years; range,19-50 years). Inclusion criteria were intact maxillary jaws with no more than a 1 tooth missing per quadrant (excluding third molars) and without evidence of any preexisting craniofacial dysmorphology (determined by inspection or listed in the health history on file, if present).
The skulls were imaged with a state-of-the-art cone-beam computed tomography unit (CB Mercuray, Hitachi Medical, Tokyo, Japan) at a 9-in field of view, 100 kVp, and 10 mA. The resulting voxel size was 0.28 mm. The software used was Accurex (Cybermed, Seoul, Korea).
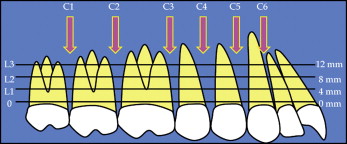
Six interdental sites on each side were surveyed in this study, from the mesial aspect of the maxillary canine to the distal aspect of the maxillary second molar, and measurements were taken at 3 levels ( Fig 2 ), creating 18 measurement sites.
The images were oriented as follows.
- 1.
By using the sagittal view, the axial plane was oriented parallel to the palatal plane and adjusted to approximately midroot level.
- 2.
By using the axial view, the coronal plane was adjusted to section through the alveolar process at 90° to the palatal bone surface bisecting the interradicular site ( Fig 3 ).
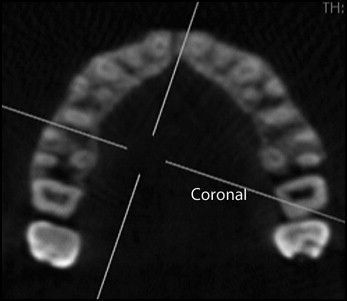
Fig 3 Axial slice of alveolar process illustrating the interdental sites and the orientation of the coronal slice at the site being surveyed. - 3.
A clear section of the alveolar process appeared as a result in the coronal view, on which measurements of cortical bone thickness and bone depth were created at 4, 8, and 12 mm (levels 1-3) from the alveolar crest, and again at 90° to the surface of the bone ( Fig 4 ). The alveolar crest level was defined as 1 mm apical to the cementoenamel junction of the adjacent teeth.
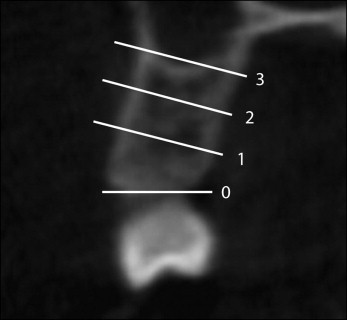
Fig 4 Coronal slice illustrating the measurement levels.
Cortical bone thickness was defined as the buccolingual dimension of the palatal cortical bone measured perpendicular to the bone surface from its outer surface to the demarcation of cortical and cancellous bones ( Fig 5 ). The cutoff lines between bone and air, and cortical bone and cancellous bones, were determined visually with gray-white discrimination and drawn manually as described by Baumgaertel.
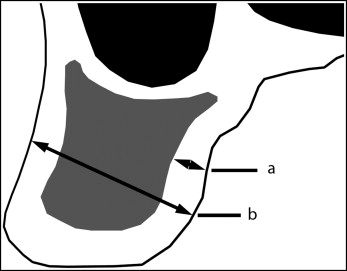
Bone depth was defined as the total amount of bone available in the buccolingual direction measured from the palatal surface of the alveolar process to either the buccal surface of the alveolar process or the inner surface of the maxillary sinus, depending on the measurement level. Measurements were also taken at 90° to the palatal bone surface ( Fig 5 ).
Statistical analysis
SPSS software (version 17.0; SPSS, Chicago, Ill) was used for all statistical analyses, and significance levels for all tests were set at P ≤0.05. Preliminary data analysis suggested normal frequency distribution (Shapiro-Wilk test) and equality of variances (Levene’s test). Intraclass correlation was used to determine the reliability of the measurement method: on 10 slices on 10 skulls, all measurements (cortical bone thickness and bone depth) were repeated twice, 6 months apart. The paired Student t test was used for additional preliminary data analysis to test for differences between the left and right sides. No statistically significant differences were found, so the data were pooled. Two-way repeated measures analysis of variance (ANOVA) was used to evaluate the influence of interdental site and measurement level on cortical bone thickness and bone depth.
Results
Intraclass correlations (r = 0.88 for cortical bone thickness; r = 0.99 for bone depth) suggested high reliability for both measurements.
Cortical bone thickness was generally thinnest at level 3 (1.17 ± 0.33 mm) and thickest at level 2 (1.26 ± 0.30 mm). The interdental site with the least overall cortical bone thickness was located distal to the second molar (1.06 ± 0.26 mm), and the interdental site with the greatest overall cortical bone thickness was located between the canine and the first premolar (1.33 ± 0.32 mm). Cortical bone thickness ranged from a mean of 1.0 mm (±0.27 mm) at contact 2, level 3 to a mean of 1.38 mm (±0.26 mm) at contact 4, level 2 ( Table II ).
| Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Measurement level | ||||
| L1 | 1.2 | 0.30 | 0.42 | 2.63 |
| L2 | 1.26 | 0.30 | 0.54 | 2.13 |
| L3 | 1.17 | 0.33 | 0.3 | 2.2 |
| Interdental site | ||||
| C1 | 1.06 | 0.27 | 0.3 | 1.88 |
| C2 | 1.11 | 0.3 | 0.4 | 2.13 |
| C3 | 1.16 | 0.28 | 0.55 | 1.9 |
| C4 | 1.28 | 0.29 | 0.49 | 2.16 |
| C5 | 1.33 | 0.32 | 0.63 | 2.63 |
| C6 | 1.3 | 0.31 | 0.42 | 2.13 |
| Measurement site | ||||
| C1L1 | 1.1 | 0.23 | 0.68 | 1.58 |
| C1L2 | 1.1 | 0.27 | 0.57 | 1.88 |
| C1L3 | 1.0 | 0.28 | 0.30 | 1.75 |
| C2L1 | 1.09 | 0.28 | 0.43 | 1.74 |
| C2L2 | 1.25 | 0.31 | 0.54 | 2.13 |
| C2L3 | 1.0 | 0.27 | 0.40 | 1.80 |
| C3L1 | 1.14 | 0.29 | 0.55 | 1.80 |
| C3L2 | 1.11 | 0.24 | 0.57 | 1.60 |
| C3L3 | 1.23 | 0.30 | 0.67 | 1.90 |
| C4L1 | 1.22 | 0.26 | 0.70 | 1.80 |
| C4L2 | 1.38 | 0.26 | 0.79 | 1.82 |
| C4L3 | 1.22 | 0.31 | 0.49 | 2.16 |
| C5L1 | 1.35 | 0.33 | 0.76 | 2.63 |
| C5L2 | 1.39 | 0.29 | 0.75 | 1.90 |
| C5L3 | 1.27 | 0.34 | 0.63 | 2.20 |
| C6L1 | 1.29 | 0.33 | 0.42 | 2.13 |
| C6L2 | 1.34 | 0.29 | 0.63 | 1.94 |
| C6L3 | 1.28 | 0.31 | 0.60 | 1.97 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


