Multiplanar imaging is a fairly new concept in diagnostic imaging available with a number of contemporary imaging modalities such as CT, MR imaging, diagnostic ultrasound, and others. This modality allows reconstruction of images in different planes (flat or curved) from a volume of data that was acquired previously. This concept makes the diagnostic process more interactive, and proper use may increase diagnostic potential. At the same time, the complexity of the anatomical structures on the maxillofacial region may make it harder for these images to be interpreted. This article reviews the anatomy of maxillofacial structures in planar imaging, and more specifically cone-beam CT images.
The main challenge in cone beam CT (CBCT) imaging and diagnosis is the lack of familiarity experienced by most dental professionals with the concept of multiplanar imaging that is offered by this new and exciting technology. Dentists and specialists, with only a few exceptions, have a wide experience in diagnosis using the traditional dental imaging modalities (intraoral radiography and panoramic radiography), and the comfort level in their diagnostic skills with these modalities is high. These imaging modalities have been taught for several decades in the dental schools and in other training courses.
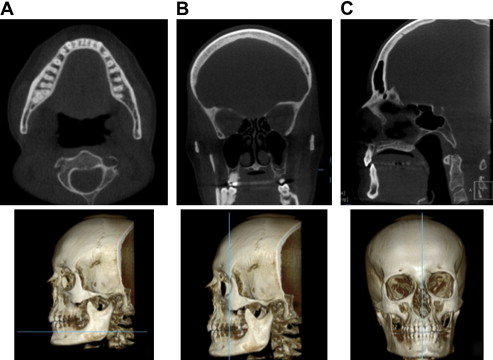
Diagnostic imaging in different planes is a new concept and may require a different view of the imaging data. It is reminded that multiplanar imaging or reformatting is the ability to generate images in different planes, flat or curved. This ability is offered only by some contemporary imaging modalities, such as CBCT, medical CT, MRI, ultrasound, and others. Because a volume of data has been acquired and stored by CBCT, these data can be reformatted or realigned and several different types of images can be synthesized in any way the diagnostician requires. With multiplanar imaging, the diagnostician or operator can recreate images in different planes (flat or curved) with simple functions. This increases the diagnostic efficiency in the hands of the knowledgeable individual in an unparalleled way ( Fig. 1 ).
In this article, the author reviews the appearance of several anatomic structures of the maxillofacial region and the head and neck region in general; these structures are revealed in a variety of planes (eg, axial, coronal, sagittal, and more). What may add to the complexity of these images is the fact that this technology may demonstrate structures of interest, such as teeth and jaws, in a view that dental professionals have not seen in the past; dentists were never able to view the third dimension of the regions of interest. From the beginning, this may make the images look unfamiliar and different.
First, as with every other dental diagnostic image, the images are viewed as if the patient under examination were sitting opposite the dentist, as in the dental chair. The structures identified on the dentist’s right side would represent the anatomic structures on the patient’s left and vice versa. Most of the available software of the various manufacturers properly identifies the right and left sides or the buccal and lingual sides of the images; thus, orientation is not difficult.
The author starts with the evaluation of well-known dental structures in the maxillofacial region in cross sections. Cross-sectional images are generated perpendicular to the arch-form of the maxilla or mandible. The image demonstrated in Fig. 2 is a cross-sectional image (cut or slice) of the maxilla and mandible in the first molar location. In this image, the buccal and palatal or lingual sides are clearly identified.
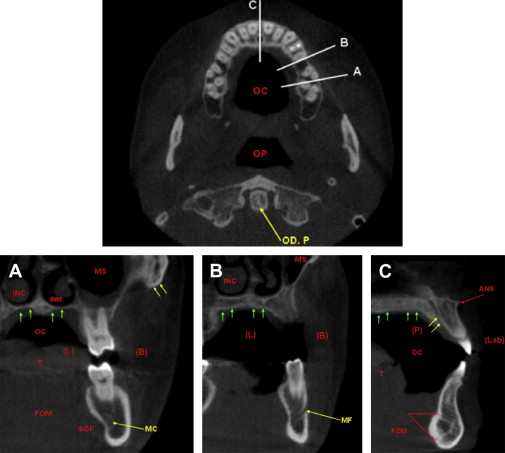
The maxillary sinus is a pyramidal in shape low-density (black or dark) structure. The appearance of healthy air cavities in the maxillary sinuses is dark (black) because of the fact that air attenuates x-rays minimally. The thin cortical outline of the buccal and medial sinus walls can be identified in these images. The medial wall of the maxillary sinus borders the sinus cavity from the nasal cavity. Note the soft tissue coverage of the nasal cavity being demonstrated as gray in the image. The high-density core is the inferior nasal concha. The reader is reminded that the inferior nasal concha is an independent facial bone, whereas the rest of the conchae, middle and superior nasal conchae, are parts of the ethmoid bone. Also note that the soft tissue in the region (intraoral and extraoral) demonstrates an almost uniform density; CBCT soft tissue contrast is not adequate to demonstrate differences in musculature or fat, for example.
Further inferior in the same image, you can identify a cross section of the mandibular molar region and the long axis of the mandibular bone in the cross section. Note that the mandibular teeth are not always parallel with the long axis of the mandibular bone in the cross section. The cortical outline of the mandibular bone appears to be much thicker than that of the maxilla (discussed previously). Moreover, the submandibular gland fossa sometimes is more prominent than others. This undercut can be rather severe at times and may impose an anatomic limitation in implant placement in the region. Last, significant anatomic structures, such as the lingual artery, are passing nearby. The mandibular canal is identified into the mandibular bone.
As we move more anteriorly, we are examining cross-sectional images in the premolar locations. You can see similar anatomic structures as the ones before; however, the further anterior we go, the narrower the maxillary sinuses become because we are approaching the anterior wall of the maxillary sinuses. In this cross section, we can see the anterior opening of the mandibular canal, which is the mental foramen. There is considerable variation in the appearance of the mental foramen and its emergence angle (opening angle) into the buccal aspect of the mandibular bone.
The next cross section is along the midline of the maxilla and the mandible, and some different anatomic structures are seen: in this case, the floor of the nasal cavity and the nasopalatine canal. The reader is reminded that the nasopalatine canal starts from the floor of the nasal cavity (inferior meatus) with dual foramina (superior foramina). It carries branches of the nasopalatine nerve, which exit the canal through the incisive foramen and spread to the anterior aspect of the hard palate (see Fig. 2 C). The nasopalatine canal may vary in dimensions, and also may pose a limitation in placing implants in this aesthetic zone, the anterior maxilla.
Once more, great variation exists concerning the shape of the anterior mandible in cross sections. A significant anatomic structure in the lingual aspect of the mandibular bone, along the midline of the mandible, is the lingual foramen or foramina, which accommodate the terminal branches of the lingual artery (see Fig. 2 C; Fig. 3 ). Often, they are closely associated with the genial tubercles (high-density structures), which serve as muscle attachment points. The diameter of these canals or foramina is related to the blood-supplying capacity of the blood vessel, and as a result, if they are wide enough, they may bleed significantly if injured during surgical procedures, such as implant surgery . Despite the fact that they are located toward the inferior third of the mandibular bone, they may be seen closer to the crest pending atrophy of the anterior alveolar ridge.
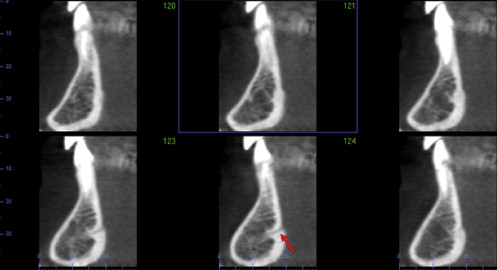
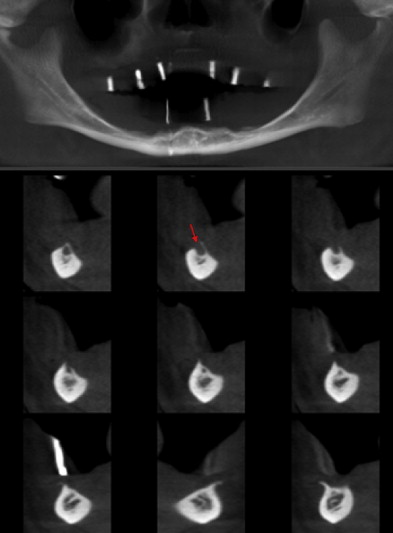
Additional vascular canals are noted from time to time in the mandibular bone anterior to the premolar locations in a region that generally is considered to be a safe site for implant placement (interforaminal region). These canals often represent accessory lingual foramina that host accessory branches of the lingual artery. Depending on the width, they may also pose limitations for surgical procedures . Once more, these foramina are identified fairly inferior, unless severe bone resorption is noted ( Fig. 4 ).
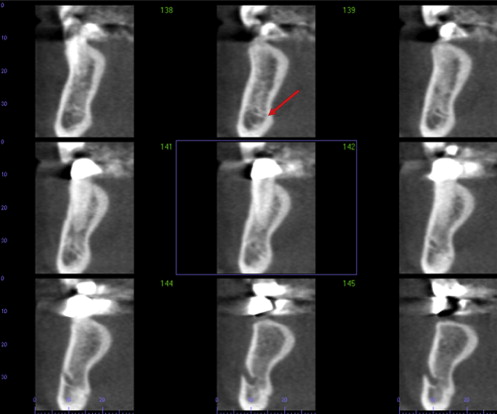
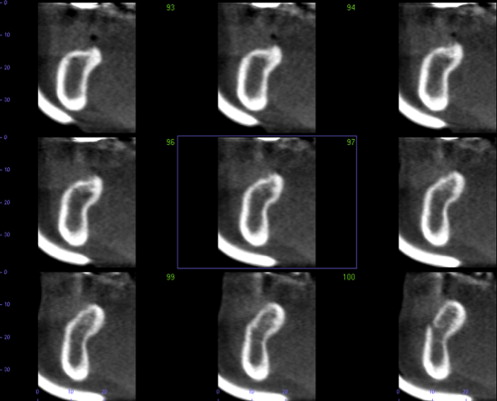
The variation of the shape and size of the alveolar ridge is remarkable. After tooth extraction, the maxillary bone and mandibular bone rarely remain unchanged. Frequently, the edentulous areas are accompanied by undercuts as a result of bone resorption, and these undercuts may pose anatomic limitations in implant placement in the posterior mandible ( Figs. 5 and 6 ).
The reader has now become familiar with the cross-sectional imaging of the major anatomic structures in the oral cavity that the dentist frequently uses and identifies in routine dental radiographs. The author now examines these anatomic structures among others in different planes: axial, coronal, and sagittal planes. Once more, these images are reviewed as if the patient were opposite the dentist. Consequently, the right side of the patient’s face or the right anatomic structures are on the dentist’s left and vice versa. Axial sections (cuts) are the images that have been generated perpendicular to the long axis of the human body (the long axis of the head in this case). These images section the teeth perpendicular to their long axis; as a result, the dentist is able to see transverse sections of the roots and crowns of the teeth in the areas of interest.
Axial images are excellent for the evaluation of the visible parts of the neck and cervical spine, integrity of the palatal and buccal cortical plates of the maxillary and mandibular dentition, lateral and medial wall of the sinuses, lateral walls of the nasal cavity, anatomic structures in the nasal cavity, zygomatic bones and zygomatic arches, and skull base, for example.
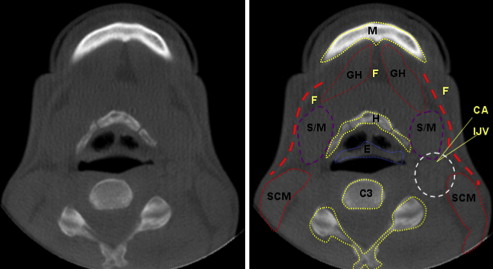
Only parts of the patient’s neck can be visualized toward the inferior end of the imaging volume. Soft tissue structures are mostly present at that level ( Fig. 7 ). The inferior border of the anterior mandible may be sectioned at this level and may be visualized toward the superior border of the image. The hyoid bone and the body and the processes of the C3 to C4 vertebrae are expected to be seen in the same cuts. The soft tissue structures identified in this image include the sternocleidomastoid muscles bilaterally, the geniohyoid muscles, and the submandibular salivary glands. In the center of the image, this semicircular low-density (dark structure) in the middle of the image represents the patient’s airway. The airway is separated almost in two halves by a soft tissue structure that is crescent in shape (and some times irregular in appearance), the epiglottis. Approximately at this level, the common carotid artery bifurcates into two main branches, the internal carotid and external carotid arteries, which supply the brain and face of each side, respectively. The most reliable reported landmarks to indicate the level at which bifurcation occurs are the C3 and C4 levels and the superior border of the thyroid cartilage of the larynx; however, variation is not uncommon (see Fig. 7; Fig. 8 ). Superior to the bifurcation, the blood vessels are less distinguishable because of their reduced diameter.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


