Cone-beam CT (CBCT) is useful for many maxillofacial applications, such as implant site imaging and diagnosis and treatment planning for orthodontics and craniofacial surgery. Dentoalveolar applications, such as carious lesion detection and characterization, assessment of the three-dimensional nature of periodontal bone topography, and various endodontic applications are less known and not as thoroughly studied. This article explores and assesses in vivo and in vitro efforts to apply CBCT imaging to these more common dentoalveolar tasks. CBCT imaging, like its medical counterpart, can be seen as a highly useful and, in some instances, indispensable part of the dental imaging armamentarium.
In this issue of Dental Clinics of North America , cone-beam computed tomography (CBCT) applications in dentistry are examined. This article focuses on applications of CBCT to dentoalveolar disease and conditions, as applied in the practice of general dentistry, periodontics, and endodontics.
The technology of CBCT is described elsewhere in this issue of Dental Clinics and will not be repeated in detail here. It suffices to say that CBCT is a new application of CT that generates three-dimensional (3D) data at lower cost and absorbed doses than conventional CT found in the practice of medical radiology. Data from the craniofacial region are often collected at higher resolution in the axial plane than those from conventional CT systems . In addition, these systems do not require a large amount of space and can easily fit into most dental practices today.
Most of the attention regarding CBCT imaging has focused on applications for dental implant placement, orthodontics, surgery, and temporomandibular joint imaging , and not as much emphasis has been placed on the applications of CBCT to dentoalveolar conditions and treatment. This article reviews and examines the available evidence from the clinical and scientific literature pertaining to dentoalveolar tasks, primarily limited to three basic areas: (1) caries diagnosis, (2), detection and characterization of the bony aspects of periodontal disease, and (3) endodontic applications, including the diagnosis of periapical lesions due to pulpal inflammation, visualization of canals, elucidation of internal and external resorption, and detection of root fractures.
The chief limitation of current conventional intraoral and panoramic imaging for these common dentoalveolar diseases is the problem of conspicuity , which is largely the result of the representation of a 3D structure depicted by a two-dimensional (2D) image. This limitation is true for caries and periodontal and endodontic applications . Dentistry has largely used the same method of 2D imaging since the first intraoral radiograph obtained in 1896. In fact, on close examination, only one or two significant advances in dental imaging have been made since then. These advances include panoramic imaging and tomography, with the former being far more useful for dental applications, and the latter historically being limited primarily to temporomandibular joint and implant site imaging. Digital imaging has been an advancement, yet the imaging geometry has not changed with these commonly used intraoral and panoramic technologies.
Earlier attempts have been made to improve the diagnosis and treatment of dentoalveolar conditions with 3D imaging using variations of tomosynthesis, most notably, tuned aperture CT (TACT) imaging . Although TACT provided some incremental benefit for periodontal and endodontic applications, improvements in caries detection and characterization were limited to simulated recurrent caries . These tomosynthetic methods proved promising but thus far have found limited application in the practice of dentistry. A new type of tomosynthetic technology, based on statistical inversion methods, named volume tomography, has recently entered the dental imaging market and may prove useful. It produces a stack of 256 images depicting cross-sectional information useful for implant treatment planning, which can visualize a limited volume of 6.0 by 6.0 cm. The system is an option with an OP 200 panoramic unit (Instrumentarium Dental, Tuusula, Finland) and is lower in cost and radiation dose than CBCT systems.
By the end of the twentieth century and the beginning of the twenty-first, it has become apparent that CBCT imaging may indeed be the next major advancement in dentoalveolar imaging, providing true 3D imaging at a lower cost than conventional CT, with radiation risks similar to current methods of intraoral imaging, including panoramic and full-mouth radiographic examination . The advantages of CBCT for other maxillofacial applications have been well documented in this issue of Dental Clinics. What follows is a review of what is known about the potential benefits of CBCT imaging as applied to dentoalveolar tasks defined in this article as caries diagnosis, characterization of periodontal lesions, and various endodontic applications.
When considering a comparison of different imaging technologies, the reader is reminded that an increase in efficacy or lack thereof does not necessarily imply superiority or inferiority. Other factors must also be considered. A consideration of the total radiation risks for current imaging modalities, and ease of use and efficiency, should be considered. An example would be comparing CBCT with a full-mouth series of intraoral radiographs for the detection of dentoalveolar disease. CBCT would not necessarily have to demonstrate a superior diagnostic efficacy over a conventional full-mouth series of radiographs in order to be considered an improvement over conventional methods. If CBCT was equal to a full-mouth series in efficacy, it could be argued that, depending on machine type, the radiation risk would be considerably less, as would the time and effort it takes to image the patient. The reader may conclude that CBTC, under the aforementioned conditions, would actually be considered superior to conventional intraoral imaging methods. Alternative examinations such as a panoramic, with bitewings and limited periapical radiographs, might prove to have risks equal to, or fewer than, CBCT. In addition, the presence of metal effectively eliminates the possibility of caries detection in restored teeth, so CBCT may not prove practical for many patients as a general dental examination method unless it is supplemented with bitewing radiographs. Finally, in vitro studies involve no patient motion. Motion can, and often does, lead to CBCT image degradation. With these considerations in mind, the current literature on CBCT for caries diagnosis, periodontal bone characterization, and endodontic applications is examined, followed by a summary of what we know and can apply to current dental practice now and in the future.
Caries diagnosis
The detection of proximal and occlusal surface caries by conventional intraoral 2D methods has demonstrated only low-to-moderate sensitivity, but slightly better specificity, and high observer variability . Pervious extraoral imaging methods for caries detection have met with limited success and dubious clinical applications. CBCT imaging appears to be the best prospect for improving the detection and depth assessment of caries in approximal and occlusal lesions. Recent work with benchtop-based local or limited CBCT (LCT) systems has demonstrated the potential for caries detection and depth characterization by high-resolution systems . All five studies used a benchtop CBCT system with a high resolution (40-μm pixel) charge-coupled device (CCD) detector and rotating turntable with a fixed anode intraoral radiograph source; they also used histologically generated ground truth and small sample sizes of 24 to 30 teeth. LCT images were presented in parasagittal (similar to the bitewing view) and axial planes and were compared with bitewing radiographs. General linear model and receiver operating characteristic curves with analysis of variance methods were the statistical methods used. Kalathingal and colleagues found no difference in the detection of carious lesions but did find that LCT was superior for caries depth assessment and although sensitivity increased, specificity showed no difference. The work performed by van Daatselaar and coworkers demonstrated the superiority of LCT images for caries detection and noted that the number of source images could be as low as 14, a significant finding because a CCD detector was used for the study.
Turning to clinical CBCT systems, Akdeniz and coworkers and Tsuchida and colleagues used a limited-volume CBCT (LCBCT) Accuitomo device and compared in vitro CBCT results with either conventional film radiography or storage phosphor (SP) images. Akdeniz and colleagues, using 41 teeth, histologically verified ground truth, and all image planes for viewing found that LCBCT was superior for caries depth assessment when compared with SP and film. These results corroborated the work of Kalathingal and colleagues . One possible weakness of the study was its use of only two observers.
Tsuchida and colleagues used micro-CT verified ground truth on 50 teeth with noncavitated incipient lesions, in a study where only 29 of the 100 surfaces were sound. Seven observers were used to generate receiver operating characteristic curves, which demonstrated no significant differences between the LCBCT images and film. This finding is not surprising, considering the difficulty of detecting incipient lesions.
A most recent and thorough study using full-volume CBCT and LCBCT by Haiter-Neto and colleagues compared the NewTom 3G system (APF Imaging, Elmsford, New York) using three fields of view (12, 9, and 6 inches), the Accuitomo LCBCT system (J. Morita Manufacturing Corporation, Kyoto, Japan), Insight film (Eastman Kodak Company, Rochester, New York), and Digora SP (Soredex, Tuusula, Finland) images for the detection of approximal and carious lesions. Ground truth was histologically determined with 63% sound surfaces for approximal lesions and 6% for sound surfaces, with the former being the most realistic distribution of lesions to date which actually approximates interproximal caries prevalence. Six observers viewed all three fields of view for the NewTom system and all other modalities. The results showed that the NewTom 12-inch and 9-inch images had significantly lower sensitivities than the Accuitomo systems, whereas the NewTom 9-inch and 6-inch images had significantly lower specificities than the insight film and Digora images. The Accuitomo images were determined to be no different from film or the Digora-based images. For occlusal surfaces, the Accuitomo presented a higher sensitivity than the other systems. Specificity and overall true score did not differ among the modalities for occlusal lesions. The investigators concluded that the NewTom 3G system had a lower diagnostic accuracy for caries detection than the intraoral or LCBCT systems. The LCBCT systems were determined to be equal to the intraoral systems but did score higher in detecting dentinal lesions. These results are not surprising, given the lower spatial resolution of the NewTom system and the higher signal to noise ratio of the LCBCT system. Typically, the sensitivities were higher for the CBCT modalities but specificities were less, suggesting that one of the limitations of caries detection with CBCT imaging may be an increase in the number of false-positives. The investigators reminded the readers that CBCT doses for caries detection are still higher for many types of intraoral examinations, although they vary significantly, depending on which country is being studied. For instance, in the United States, a full-mouth series of radiographs with D speed film and no rectangular collimation is the most common type of full-mouth radiographic examination. CCD-based, or even F speed with rectangular collimation, image series will be significantly less. Thus, the risks for CBCT imaging as a possible replacement for a full series of radiographs vary, depending on the system with which it is being compared.
The study did not separate the occlusal from the approximal lesions. Further studies are needed to evaluate CBCT for the detection of occlusal or pit and fissure caries, a task for which 2D imaging has been weak. In addition, the reader is reminded that in the in vitro studies mentioned earlier, intraoral 2D images were usually obtained under ideal geometry conditions with no closed contacts, cone cuts, or projective distortions. The equivalence of CBCT scores to those of 2D imaging may, in the minds of some, demonstrate the superiority of the former system. This point will also be considered in the conclusions. At this time, the application of CBCT imaging to caries diagnosis is promising, with more research needed, especially in vivo investigations. In addition, with current technology, it is assumed that teeth with metal or even radiopaque restorations should not be considered for CBCT caries imaging.
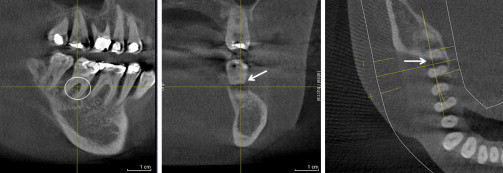
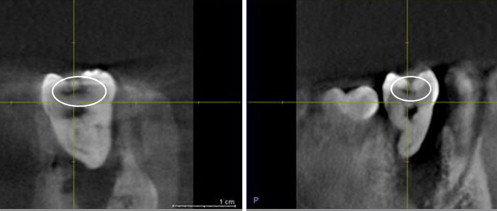
Examples of CBCT for caries imaging can be seen in Figs. 1 and 2 .
Periodontal applications
In his 2004 summary of periodontal imaging methods in Periodontology , Mol states, “Relatively few technologies have emerged to address the critical needs in periodontal diagnosis” . He goes on to point out that although digital imaging has added value to intraoral imaging, an increase in diagnostic capabilities has not been one of the benefits. Mol discusses the limitations of extraoral imaging (panoramic) with its associated drawbacks but does point out the usefulness in association with bitewings and selected periapicals. Mol also reviews the more advanced digital technologies, such as TACT, digital subtraction, and conventional CT scanning, and states their potential for an increase in diagnostic efficacy and characterization of the periodontal bone status. He concludes by outlining the practical limits of these technologies and explains why they are not going to be particularly useful in the practice of dentistry . Previous studies have shown that CT assessment of alveolar bone height and bony pockets is reasonable, accurate, and precise . Mol states that CBCT studies applied to periodontal imaging were in progress and not available at the time of publication of his review. Several of these studies are now available. Most studies investigating the application of CBCT imaging to periodontal bone status are in vitro, although a few are in vivo, with either full-volume CBCT or limited-volume units used.
Vandenberghe and coworkers investigated periodontal bone architecture using 2D CCD and 3D full-volume CBCT-based imaging modalities. Periodontal bone levels and defects were assessed and evaluated against two human skulls’ gold standard. Visualization of lamina dura, crater defects, furcation involvements, contrast, and bone quality were also evaluated. They concluded that CBCT image measurements of periodontal bone levels and defects were comparable to intraoral radiography. It was found that CBCT images demonstrated more potential in the morphologic description of periodontal bone defects and conversely, the CCD images provided more bone details. Using a dry skull with artificial defects and full-volume CBCT, Misch and colleagues found similar results. Their investigation demonstrated that CBCT was as accurate as direct measurements using a periodontal probe and as reliable as radiographs for interproximal areas. In measurements of buccal and lingual defects, CBCT proved superior to conventional radiography. Because of this finding, the investigators concluded that CBCT offered a significant advantage over conventional radiography.
In a 2005 study using human and pig material, Mengel and coworkers investigated the use of CBCT in the diagnosis of periodontal defects using intraoral radiography, panoramic radiography, CT, and LCBCT in comparison with histologic specimens. It was demonstrated that all intrabony defects could be measured in three planes in the CT and LCBCT scans with great accuracy true to scale, whereas only mesial, distal, and craniocaudal plane defects could be detected by intraoral and panoramic imaging. It was also concluded that the LCBCT system produced higher-quality images. Noujeim and coworkers found similar results when using the LCBCT system to detect simulated interradicular lesions of varying depth in comparison with intraoral radiography. Two studies in linear accuracy have recently been published by Loubele and colleagues and Mol and colleagues . Loubele and coworkers designed a study to compare the accuracy of LCBCT with multislice CT for linear measurements with caliper-determined measurements using cadaveric materials. They concluded that both systems were accurate with submillimeter measures. In a study directed more to periodontal defects, Mol, using an older form of CBCT using a full field of view, found that CBCT images provided better diagnostic and quantitative information on periodontal bone levels in three dimensions than conventional radiography. The study also demonstrated a limitation in that the accuracy in the anterior aspect of the jaws was limited. The system used a NewTom 9000 unit (APF Imaging, Elmsford, New York), generating images that were inferior in quality to what more up-to-date systems can generate.
The fact that these studies used full-volume CBCT and limited-volume systems hints that either system may be more capable than intraoral radiography in the visualization of periodontal bone architecture. The reader is reminded that motion can cause image degradation and that all the studies mentioned are in vitro and are not subject to the less than ideal clinical situation . At the same time, intraoral radiography is featured in ideal conditions in these in vitro studies.
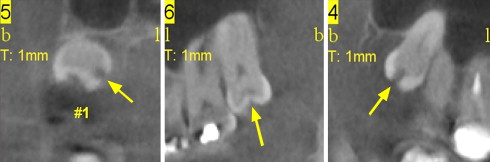
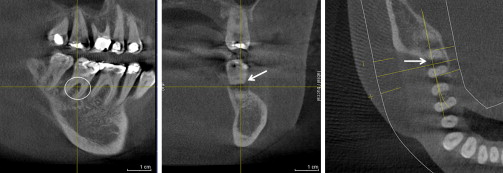
In a recent review of currently published literature on CBCT for periodontology, Kasaj and Willershausen conclude that the low dosage and superior image quality in comparison with conventional CT are promising for periodontal applications, especially in the areas of intrabony defects, dehiscence and fenestration defects, and periodontal cysts, and in the diagnosis of furcation-involved molars. This summary encapsulates the findings of the studies discussed earlier. Overall, these studies suggest that CBCT imaging has the potential to replace intraoral imaging for the assessment of periodontal architecture. However, clinical studies would be helpful in supporting this conclusion. CBCT may be a useful and more practical clinical tool than digital subtraction radiography for the assessment of changes in periodontal bone over time. Examples of CBCT for periodontal imaging can be seen in Figs. 3 and 4 .
Periodontal applications
In his 2004 summary of periodontal imaging methods in Periodontology , Mol states, “Relatively few technologies have emerged to address the critical needs in periodontal diagnosis” . He goes on to point out that although digital imaging has added value to intraoral imaging, an increase in diagnostic capabilities has not been one of the benefits. Mol discusses the limitations of extraoral imaging (panoramic) with its associated drawbacks but does point out the usefulness in association with bitewings and selected periapicals. Mol also reviews the more advanced digital technologies, such as TACT, digital subtraction, and conventional CT scanning, and states their potential for an increase in diagnostic efficacy and characterization of the periodontal bone status. He concludes by outlining the practical limits of these technologies and explains why they are not going to be particularly useful in the practice of dentistry . Previous studies have shown that CT assessment of alveolar bone height and bony pockets is reasonable, accurate, and precise . Mol states that CBCT studies applied to periodontal imaging were in progress and not available at the time of publication of his review. Several of these studies are now available. Most studies investigating the application of CBCT imaging to periodontal bone status are in vitro, although a few are in vivo, with either full-volume CBCT or limited-volume units used.
Vandenberghe and coworkers investigated periodontal bone architecture using 2D CCD and 3D full-volume CBCT-based imaging modalities. Periodontal bone levels and defects were assessed and evaluated against two human skulls’ gold standard. Visualization of lamina dura, crater defects, furcation involvements, contrast, and bone quality were also evaluated. They concluded that CBCT image measurements of periodontal bone levels and defects were comparable to intraoral radiography. It was found that CBCT images demonstrated more potential in the morphologic description of periodontal bone defects and conversely, the CCD images provided more bone details. Using a dry skull with artificial defects and full-volume CBCT, Misch and colleagues found similar results. Their investigation demonstrated that CBCT was as accurate as direct measurements using a periodontal probe and as reliable as radiographs for interproximal areas. In measurements of buccal and lingual defects, CBCT proved superior to conventional radiography. Because of this finding, the investigators concluded that CBCT offered a significant advantage over conventional radiography.
In a 2005 study using human and pig material, Mengel and coworkers investigated the use of CBCT in the diagnosis of periodontal defects using intraoral radiography, panoramic radiography, CT, and LCBCT in comparison with histologic specimens. It was demonstrated that all intrabony defects could be measured in three planes in the CT and LCBCT scans with great accuracy true to scale, whereas only mesial, distal, and craniocaudal plane defects could be detected by intraoral and panoramic imaging. It was also concluded that the LCBCT system produced higher-quality images. Noujeim and coworkers found similar results when using the LCBCT system to detect simulated interradicular lesions of varying depth in comparison with intraoral radiography. Two studies in linear accuracy have recently been published by Loubele and colleagues and Mol and colleagues . Loubele and coworkers designed a study to compare the accuracy of LCBCT with multislice CT for linear measurements with caliper-determined measurements using cadaveric materials. They concluded that both systems were accurate with submillimeter measures. In a study directed more to periodontal defects, Mol, using an older form of CBCT using a full field of view, found that CBCT images provided better diagnostic and quantitative information on periodontal bone levels in three dimensions than conventional radiography. The study also demonstrated a limitation in that the accuracy in the anterior aspect of the jaws was limited. The system used a NewTom 9000 unit (APF Imaging, Elmsford, New York), generating images that were inferior in quality to what more up-to-date systems can generate.
The fact that these studies used full-volume CBCT and limited-volume systems hints that either system may be more capable than intraoral radiography in the visualization of periodontal bone architecture. The reader is reminded that motion can cause image degradation and that all the studies mentioned are in vitro and are not subject to the less than ideal clinical situation . At the same time, intraoral radiography is featured in ideal conditions in these in vitro studies.
In a recent review of currently published literature on CBCT for periodontology, Kasaj and Willershausen conclude that the low dosage and superior image quality in comparison with conventional CT are promising for periodontal applications, especially in the areas of intrabony defects, dehiscence and fenestration defects, and periodontal cysts, and in the diagnosis of furcation-involved molars. This summary encapsulates the findings of the studies discussed earlier. Overall, these studies suggest that CBCT imaging has the potential to replace intraoral imaging for the assessment of periodontal architecture. However, clinical studies would be helpful in supporting this conclusion. CBCT may be a useful and more practical clinical tool than digital subtraction radiography for the assessment of changes in periodontal bone over time. Examples of CBCT for periodontal imaging can be seen in Figs. 3 and 4 .