Introduction
The purposes of this study were to evaluate and compare the dentoskeletal changes concurrent with 4-point bone-borne and tooth-borne rapid maxillary expanders in growing children.
Methods
The study was conducted with 20 growing girls (ages, 12 ± 0.6 years) with posterior crossbite. They were divided into 2 equal groups; patients in one group were treated with a tooth-borne maxillary hyrax expander (TBME), and those in the other group received a bone-borne maxillary hyrax expander (BBME) anchored directly to the palatal bone. Changes were assessed using cone-beam computed tomography. Images were taken before and immediately after expansion.
Results
Superimpositions of the 3-dimensional palatal images showed significant increases in skeletal widths at the canine, first premolar, and first molar areas in both groups. The TBME group had greater nasal width expansion. Regarding the transverse dentolinear measurements, significant increases were seen in both groups, whereas the TBME group showed a greater increase than the BBME group. Significant increases in the dentoangular measurements were seen in the TBME group only and were significantly greater than in the BBME group at the first premolars.
Conclusions
There were significant increases in facial and maxillary widths for the BBME group and in nasal width for the TBME group. Both expanders produced basal bone expansion at the level of the hard palate. The TBMEs produced more dental expansion, buccal rolling, and a greater increase in nasal width than did the BBMEs.
Highlights
- •
We studied 4-point bone-borne and tooth-borne maxillary expansion in children.
- •
Basal bone expansion at the level of the hard palate was seen in both groups.
- •
Facial and maxillary widths increased more in the bone-borne group.
- •
Dental expansion and nasal width increased more in the tooth-borne group.
Maxillary constriction is considered one of the most common orthodontic problems that could be accompanied by unilateral or bilateral posterior crossbite, narrow nasal cavity, and dental crowding. Transverse maxillary deficiencies may give rise to several clinical manifestations such as maxillary hypoplasia, asymmetrical facial growth, positional and functional mandibular deviations, altered dentofacial esthetics, adverse periodontal responses, unstable dental tipping, and other functional problems.
Posterior crossbite is one of the most prevalent malocclusions; it is reported to occur in 8% and 22% of patients and requires early intervention to coordinate the maxillary and mandibular arches. The main treatment modality was introduced into orthodontics by Derichsweiler and Haas for correction of severe crossbite and improvement of nasal breathing. The primary goal of maxillary expansion was to maximize dentofacial orthopedics and minimize orthodontic movements of the teeth. In tooth-borne expanders, transmitting the expansion forces throughout the teeth might decrease the amount of force applied to the maxilla and contribute to more undesirable effects toward the anchorage teeth. However, applying expansion forces directly toward the palatal bone would provide more parallel displacement of the maxillary shelves with no unwanted tooth movement.
Many mechanically rigid fixed rapid maxillary expansion appliances have been developed to split the midpalatal suture. Hyrax (or Biederman) expanders are known for greater hygiene and comfort, minimal interference with speech, and few lesions of the palatal mucosa. However, many limitations have been identified because of their limited skeletal effects, and the potential for undesirable tooth movement, buccal tipping, and root resorption.
With the innovation of implants, a paradigm shift has occurred to the anchorage perspective, and it has been possible to reinforce anchorage during rapid maxillary expansion without dental support. Miniscrews have been used as a means of absolute orthodontic anchorage. Bone-anchored palatal expanders were claimed to transmit the expansion forces directly to the palatal bone, contributing to more skeletal movement rather than to bending of the maxillary alveolar shelves. This may allow for more physiologic sutural expansion, reduce negative dental effects, and contribute toward more efficient mechanics. The studies that used fixed palatal distractors screwed into the palatal bone and osteosynthesis reported good skeletal effects combined with protection of teeth from buccal rolling, root resorption, and bony dehiscence.
The success of rapid palatal expansion treatment depends on the appliance design, the mode of activation, and the patient’s age. Accordingly, applying this treatment before the pubertal growth peak would contribute to a more significant adaptation to the expansion therapy at the skeletal level in both maxillary and circummaxillary structures.
Studies on rapid maxillary expansion have analyzed the transverse skeletal effects of expansion therapy with dental casts, posteroanterior cephalograms, and occlusal radiographs. Posteroanterior cephalograms were considered an excellent means of distinguishing the dental and skeletal effects of rapid maxillary expansion. However, all of these diagnostic approaches give 2-dimensional data of a 3-dimensional (3D) object. Furthermore, posteroanterior cephalograms are affected by head posture, landmark identifications, and quality of the radiographs. Cone-beam computed tomography (CBCT) technology has the advantages of creating 3D volumetric images, reproducing a 3D cephalometric analysis, and accurately identifying reliable 3D cephalometric hard and soft tissue landmarks.
The purposes of this study were to evaluate and compare the transverse dentoskeletal changes concurrent with 4-point bone-borne and tooth-borne rapid maxillary expanders in growing children.
Material and methods
The protocol was approved by the ethical committee of Cairo University in Egypt. Twenty growing female patients with a mean age of 12 ± 0.6 years were recruited from the outpatient clinic of the Department of Orthodontics, Faculty of Oral and Dental Medicine at Cairo University. Inclusion criteria were an apically constricted maxillary arch shown by a unilateral or bilateral posterior crossbite requiring maxillary expansion, an open midpalatal suture verified radiographically by an occlusal film, fully erupted maxillary first and second premolars and first permanent molars, and no history of orthodontic treatment. We used subjects of the same sex to exclude any gender variability. Patients whose maxillary second premolars were not erupted yet could be selected to receive the tooth-borne expander.
The sample was equally divided. The first group was treated with a tooth-borne rapid maxillary hyrax expander appliance (TBME) supported by 4 bands placed on the maxillary first premolars and first permanent molars ( Fig 1 ), whereas the second group received a bone-borne rapid maxillary hyrax expander appliance (BBME) anchored directly to the palatal bone via 4 miniscrews ( Fig 2 ). A detailed description of the treatment procedure was explained to the patients who had agreed to participate in the study, and the consent form was signed by each subject’s guardian. Standard diagnostic orthodontic records and CBCT images were taken before and immediately after expansion to evaluate the dentoskeletal changes produced by both expanders.


For the BBME group, the hyrax expander (anatomic expander type “s”; Forestadent, Pforzheim, Germany) consisted of 4 custom-made stainless steel rings (internal diameter, 3.5 mm; external diameter, 5 mm; thickness, 1.9 mm, corresponding to the head of the miniscrew) that were fitted to the heads of the 4 miniscrews (Aarhus System; MEDICON eG, Tuttlingen, Germany) of a length of 12.2 mm and a diameter of 1.5 mm, inserted palatally between the maxillary first and second premolars, and between the maxillary second premolar and first permanent molar, at a depth of 7 mm apically from the cervix of the teeth with an angulation of 50° to 70° toward the palatal cortical plate. In the BBME group, after inserting the 4 miniscrews, a rubber base impression (Hydro C putty; DETAX GmbH & Co KG, Ettlingen, Germany) was taken, and acrylic resin dough was injected into the areas denoting the miniscrews to simulate the heads of the miniscrews to which the 4 custom made stainless steel rings were attached. The 4 arms of the hyrax expander were constructed and soldered to the milled stainless steel rings. The jackscrew used was 7 mm. An expander was fitted passively into the patient’s mouth, and the patient was instructed to activate it twice a day for 11 days (overall activation, 5.5 mm). For safety, the appliance was ligated to the lingual cleats of the maxillary first permanent molars. Postexpansion CBCT images were taken once the activation protocol was completed. The expanders were consolidated on the same day.
Both before and after CBCT images were taken with a Scanora 3D machine (Soredex, Tuusula, Finland) with an exposure of 15 mA and 85 kV, and a field of view of 14.5 (diameter) × 13 (height) cm. Image reconstruction was performed with software (Invivo version 5.1; Anatomage Dental, San Jose, Calif) to obtain the 3D data.
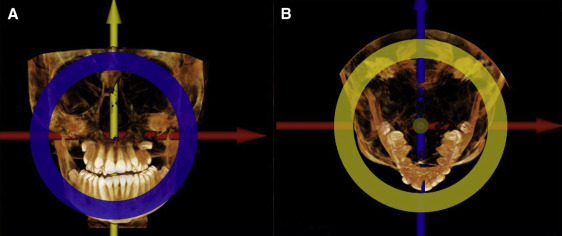
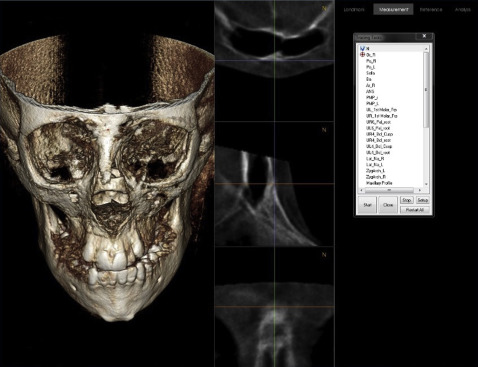
Reorientation of the patient views was performed in all 3 axes (axial, coronal, and sagittal) ( Fig 3 ). Landmark identification for all measurements was made by 2 assessors (M.I.M and another) independently. Each image was opened on 2 computers simultaneously, where fine adjustment of the position of the points was performed on the “slice locator” ( Fig 4 ). The measurements were recorded by the software and then compared to assess interobserver agreement.
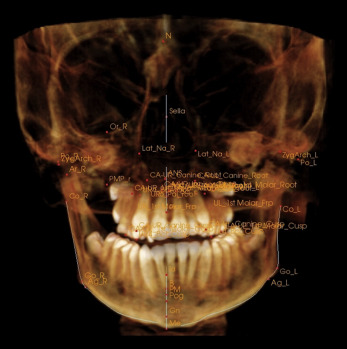
The 3D analysis was obtained by identifying the 3D reference landmarks, lines, and planes to evaluate transverse skeletal ( Fig 5 ), dentolinear ( Fig 6 ), and dentoangular measurements (in relation to the Frankfort horizontal plane) ( Fig 7 ).
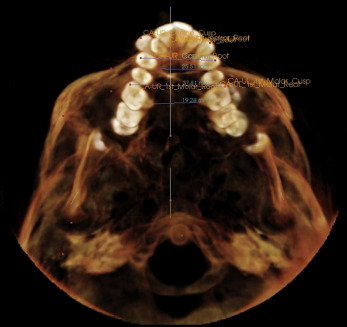
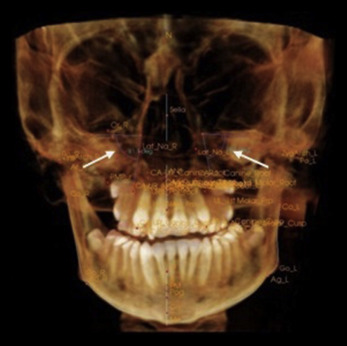
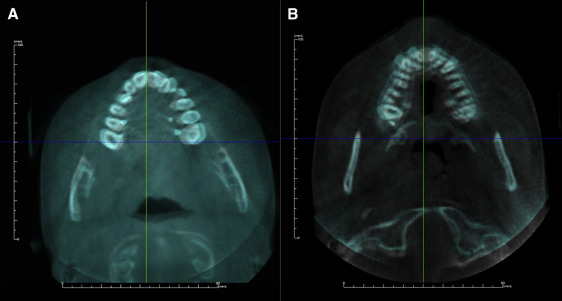
Superimposition of the hard palate was performed on the axial cut view, at the level of the tooth apices, where 3 measurements were obtained from the outer buccal cortical plate at the canine, premolar, and molar areas.
Statistical analysis
Paired t tests or Wilcoxon signed rank tests were used, according to data normality, to evaluate treatment changes. The Mann-Whitney U test was used to compare changes between the 2 groups. The significance level was set at P ≤0.05. Statistical analysis was performed with SPSS software (version 20; IBM, Armonk, NY).
A sample size calculation for this study was not done a priori; however, a post hoc analysis showed 80% power for all measurements. Although this study was not a randomized clinical trial, we believe that the risk of selection bias was low. Baseline criteria in the 2 groups were similar, as shown by the Levene test, which verified the equality of variances between the 2 groups with all P values greater than 0.05.
Results
The interobserver agreement with the Cronbach alpha test reflected good to very good interobserver agreement regarding all measurements at P = 0.001.
Superimposition showed a statistically significant increase in the skeletal palatal measurements for the BBME and TBME groups ( Table I ) in the canine, premolar, and molar areas ( Fig 8 ). Comparing the groups, we found no statistically significant difference for the mean changes ( Table II ).
| BBME | TBME | |||||
|---|---|---|---|---|---|---|
| Pretreatment Mean ± SD | Posttreatment Mean ± SD | P value | Pretreatment Mean ± SD | Posttreatment Mean ± SD | P value | |
| Skeletal maxillary and circummaxillary measurements (mm) | ||||||
| Facial width | 83.1 ± 6.3 | 89.3 ± 3.9 | 0.002 ∗ | 85 ± 7.7 | 88.9 ± 6.4 | 0.078 |
| Nasal width | 24.1 ± 2.3 | 24.7 ± 1.9 | 0.500 | 21.1 ± 1.7 | 24.6 ± 2.3 | 0.006 ∗ |
| Maxillary width | 57.4 ± 2.2 | 60 ± 3.3 | 0.039 ∗ | 57.7 ± 3.8 | 60.8 ± 6.1 | 0.112 |
| Skeletal palatal measurements (superimposition) (mm) | ||||||
| Canine area | 28.1 ± 2.4 | 30.5 ± 2.1 | 0.001 ∗ | 27.7 ± 2.9 | 31.7 ± 3.7 | 0.041 ∗ |
| Premolar area | 36.5 ± 2.4 | 39 ± 2.6 | 0.001 ∗ | 35.6 ± 4.1 | 39.6 ± 5.7 | 0.041 ∗ |
| Molar area | 48.9 ± 3.7 | 51 ± 4 | 0.001 ∗ | 45.9 ± 6.4 | 49.2 ± 7.1 | 0.004 ∗ |
| Dentolinear measurements (mm) | ||||||
| UR6-UL6 coronal | 42.6 ± 4.4 | 46.5 ± 5.5 | 0.003 ∗ | 39.8 ± 9.1 | 49.5 ± 5.7 | 0.019 ∗ |
| UR6-UL6 apical | 28.6 ± 3.7 | 32.1 ± 4.1 | 0.001 ∗ | 24.1 ± 2.7 | 27.5 ± 3.1 | 0.016 ∗ |
| UR4-UL4 coronal | 35 ± 3.2 | 37.9 ± 3.6 | 0.001 ∗ | 33 ± 3.4 | 39.7 ± 5.2 | 0.002 ∗ |
| UR4-UL4 apical | 32.9 ± 2.5 | 35.7 ± 3 | 0.001 ∗ | 30.7 ± 4.2 | 33.9 ± 3.4 | 0.003 ∗ |
| Dentoangular measurements (°) | ||||||
| UR6 BP incl | 81.9 ± 4.3 | 83.4 ± 5.3 | 0.435 | 80.3 ± 4.2 | 77.4 ± 6.1 | 0.247 |
| UL6 BP incl | 81.5 ± 4.4 | 79 ± 4.3 | 0.142 | 80.9 ± 4.3 | 75.3 ± 7.4 | 0.127 |
| UR4 BP incl | 82.9 ± 4.2 | 83.9 ± 3.2 | 0.488 | 81.8 ± 4.2 | 77.4 ± 3.7 | 0.011 ∗ |
| UL4 BP incl | 81.6 ± 6.4 | 80.8 ± 7.3 | 0.660 | 82 ± 4.2 | 76.6 ± 4.7 | 0.002 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


