Introduction
The aim of this study was to compare the time to initial alignment and extraction space closure using conventional brackets and active and passive self-ligating brackets.
Methods
One hundred adolescent patients 11 to 18 years of age undergoing maxillary and mandibular fixed appliance therapy after the extraction of 4 premolars were randomized with stratification of 2 age ranges (11-14 and 15-18 years) and 3 maxillomandibular plane angles (high, medium, and low) with an allocation ratio of 1:2:2. Restrictions were applied using a block size of 10. Allocation was to 1 of 3 treatment groups: conventional brackets, active self-ligating, or passive self-ligating brackets. All subjects were treated with the same archwire sequence and space-closing mechanics in a district general hospital setting. The trial was a 3-arm parallel design. Labial-segment alignment and space closure were measured on study models taken every 12 weeks throughout treatment. All measurements were made by 1 operator who was blinded to bracket type. The patients and other operators were not blinded to bracket type during treatment.
Results
Ninety-eight patients were followed to completion of treatment (conventional, n = 20; active self-ligating brackets, n = 37; passive self-ligating brackets, n = 41). The data were analyzed using linear mixed models and demonstrated a significant effect of bracket type on the time to initial alignment ( P = 0.001), which was shorter with the conventional brackets than either of the self-ligating brackets. Sidak’s adjustment showed no significant difference in effect size (the difference in average response in millimeters) between the active and passive self-ligating brackets (the results are presented as effect size, 95% confidence intervals, probabilities, and intraclass correlation coefficients) (−0.42 [−1.32, 0.48], 0.600, 0.15), but the conventional bracket was significantly different from both of these (−1.98 [−3.19, −0.76], 0.001, 0.15; and −1.56 [−2.79, −0.32], 0.001, 0.15). There was no statistically significant difference between any of the 3 bracket types with respect to space closure. Space-closure times were shorter in the mandible, except for the Damon 3MX bracket (Ormco, Orange, Calif), where active and total space-closure times were shorter in the maxilla. No adverse events were recorded in the trial.
Conclusions
Time to initial alignment was significantly shorter for the conventional bracket than for either the active or passive self-ligating brackets. There was no statistically significant difference in passive, active, or total space-closure times among the 3 brackets under investigation.
Although the first self-ligating bracket, the Russell lock attachment, was introduced in 1935, it is only more recently that there has been a renewed interest in the use of self-ligating brackets. Currently, 2 main types of self-ligating brackets are available, active and passive, both of which have a number of purported advantages over conventional brackets and over each other. These include fewer treatment visits, reduced overall treatment time, improved esthetics, reduced friction, improved oral hygiene, and full and secure ligation.
Previous retrospective research has shown that the use of self-ligating brackets can reduce treatment times by 4 to 6 months and by 4 to 7 visits when compared with conventional brackets. In addition, laboratory studies have suggested that friction is reduced, particularly with passive self-ligating brackets. Although improved treatment efficiency is highly desirable, it has not been a universal finding, particularly for initial alignment and space closure. Some studies have found no difference in the rate of initial alignment with either conventional or self-ligating brackets and have usually compared passive self-ligating brackets with conventional brackets. The only study to date that directly compared active with passive self-ligating brackets showed no difference in the time required to complete alignment, although there was no conventional bracket control group. Most previous researchers have also looked only at mandibular labial-segment alignment, with relatively few investigating maxillary labial-segment alignment.
Studies investigating the rate of space closure have also reported no difference between self-ligating and conventional brackets. However, they have only compared passive self-ligating brackets with conventional brackets and either have used a split-mouth design or have measured space closure for only a limited time. This has been confirmed by recent systematic reviews highlighting the variability and differences between the studies and recommending that further randomized clinical controlled trials are needed.
With these limitations in mind, the aim of this study was to investigate the time to initial alignment of both the maxillary and the mandibular labial-segment teeth along with the time to achieve space closure in the buccal segments when using 1 of 3 types of bracket: Damon 3MX passive self-ligating bracket (Ormco, Glendora, Calif), In-Ovation R active self-ligating bracket (DENTSPLY GAC International, Islandia, NY), and Omni conventional bracket (DENTSPLY GAC International). The null hypotheses were that there are no differences among the 3 bracket types during initial alignment or during space closure, or between the maxillary and mandibular arches (jaws).
Material and methods
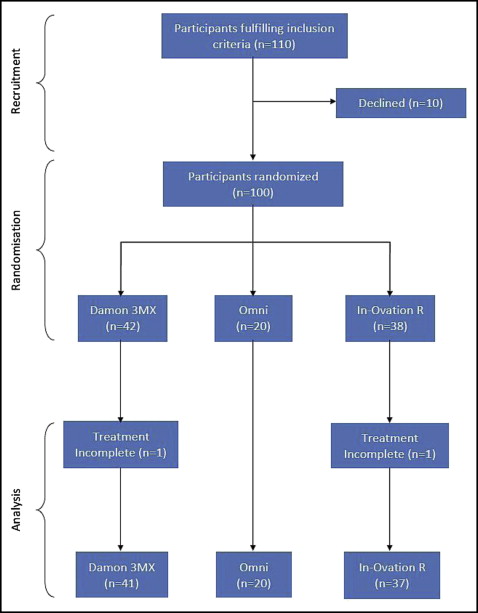
Ethical approval for the trial was granted by the ethics research committee (06/02202/6) of Taunton and Somerset Hospital, Musgrove Park, Taunton, United Kingdom. At the initial planning of this investigation, there were no studies reporting on the time to initial alignment comparing self-ligating and conventional brackets to determine a power calculation. We decided to recruit 90 subjects for the trial: 36 subjects to each self-ligating group and 18 to the conventional bracket group. However, to allow for a 10% dropout rate, 100 subjects were recruited with the following inclusion criteria: less than 18 years of age, ready to commence maxillary and mandibular fixed appliance treatment, intact labial segments, and premolar extractions required in all 4 quadrants. The principal exclusion criteria were the following: subjects who could not understand English, had learning difficulties, and had incomplete labial segments. The flow of the subjects in the trial is shown in the CONSORT diagram ( Fig 1 ), which clearly demonstrates the 3-arm parallel design with its 2:2:1 allocation ratio. In total, 100 patients were recruited into the trial, and 98 were followed to completion of treatment, with 2 dropouts. There were no outcome changes during the trial, and no interim analyses were planned or performed. When this trial began, there was less insistence on trial registration; thus, the trial and its protocol were not registered on a publicly accessible registry. No external funding was received for this trial.
All subjects were treated in the orthodontic department at Musgrove Park Hospital, Taunton, United Kingdom, by 1 of 3 consultants or 5 specialist registrars. Eligible participants and their guardians were given an information sheet before inclusion in the trial and an ample opportunity to ask any relevant questions. Block randomization was used to ensure that each participant was randomly allocated to 1 of the 3 bracket groups: the control group with conventional Omni brackets, or a self-ligation group: Damon 3MX or In-Ovation R. The randomization was carried out by the local research and development office, which was contacted by telephone before the bond-up of each participant. This process allowed allocation concealment from the researchers and prevented the possibility of prediction of the next randomization in each block. The randomization was also stratified to take into account patient age and the Frankfort mandibular plane angle. The participants were divided according to age at the start of the trial, either 11 to 14 years or 15 to 18 years. There were 3 groups for the Frankfort mandibular plane angle: low, less than 22°; average, 22° to 32°; and high, greater than 32°. This was assessed using a pretreatment lateral skull radiograph and cephalometric analysis. The block size was 10 (2 for the conventional brackets, 4 in each of the other 2 arms), and blocks were used in each of the 6 strata formed by the 2 age categories and the 3 mandibular plane angle categories.
The 3 treatment bracket groups were (1) 0.022-in slot Damon 3MX passive self-ligating brackets, (2) 0.022-in slot In-Ovation R active self-ligating brackets, and (3) 0.022-in slot Omni conventional brackets.
All brackets had a Roth prescription and were bonded using the same protocol. Molar bands (DENTSPLY GAC International) were placed on the permanent first molars; although the second molars were not routinely included in the initial bond-up, if it was required as part of the specific treatment plan, then the maxillary or mandibular second molars were bonded with second molar tubes (American Orthodontics, Sheboygan, Wis), following the same bonding protocol as used at the initial bond-up appointment.
For each subject, the same archwire sequence was used: initial archwire, 0.014-in copper nickel titanium (Ormco); second archwire, 0.018-in copper nickel titanium (Ormco); third archwire, 0.016 × 0.022-in stainless steel (DENTSPLY GAC International); and final archwire, 0.019 × 0.025-in stainless steel (DENTSPLY GAC International).
In the case of the conventional brackets, the archwires were ligated using elastomeric ligatures (OrthoCare, Bradford, United Kingdom). With the self-ligating brackets, care was taken to ensure that the clip was fully closed before progressing to the next wire size. Subjects with the Omni conventional brackets were scheduled to be seen routinely every 6 weeks, and subjects with the self-ligating brackets were scheduled to be recalled every 12 weeks as per normal practice. Initial pretreatment maxillary and mandibular alginate impressions were taken for every participant before bond-up and then were obtained every 12 weeks until completion of treatment. In each case, they were cast in dental stone within the hour. Beading wax was used to block out the brackets and archwires before the impression. This was done to facilitate easy removal of the impression and to ensure that the bracket type would remain concealed on the study models during subsequent measurements. Therefore, only the model assessor (G.S.) was blinded during the study. The patients and the operators carrying out the treatment (N.E.A., G.S., and others) could not be blinded.
Initial alignment of the maxillary and mandibular labial segments was assessed to be complete when the final 0.019 × 0.025-in stainless steel archwire was in situ and passive. At this point, the degree of passive space closure was also assessed. Active space closure was also carried out on a 0.019 × 0.025-in stainless steel archwire in both arches. Crimpable hooks were attached to the archwire between the lateral incisor and the canine brackets in each quadrant when required, and active space closure was carried out using a 150-g nickel-titanium coil spring and sliding mechanics. A passive long ligature was placed in a quadrant to prevent the space from reopening if space closure in a quadrant was complete. The use of intraoral elastics was permitted where clinically justified. This was usually once the subjects were in a stainless steel archwire. All measurements were carried out by 1 operator (G.S.). Maxillary and mandibular labial-segment alignment was measured on all participants’ study models taken at each of the nominal 12-week intervals until the end of initial alignment and the end of treatment. Little’s index of irregularity was measured in each subject using a digital Vernier caliper (Fred V. Fowler, Newton, Mass). The time to achieve total space closure was also measured using the subjects’ study models from the start of treatment and at each 12-week interval until the end of treatment with the same caliper. This was split into 2 measurements: passive space closure during the initial alignment phase and active space closure once the active space-closure mechanics were in situ. Space closure was measured from the buccal groove of the first molar to the distal contact point of the corresponding canine in each quadrant. To ensure repeatability, all measurements were made under similar conditions with a strict protocol to within 0.01 mm. Before the study, 1 researcher (G.S.) had undertaken a reproducibility study in which Little’s index and extraction space on 10 randomly selected maxillary and mandibular models were measured twice 1 week apart using the Vernier caliper. The trial was considered to be completed when all spaces were closed.
Statistical analysis
The data were analyzed using Stata software (version 12.1; Stata, College Station, Tex) with a predetermined significance level of α = 0.05. The experimental design was repeated measures with time recorded in days from the start of treatment rather than the “nominal times” in weeks when the patient was scheduled for an appointment, which was at 12-week intervals. This was therefore an intention-to-treat analysis. Since there were 98 patients, individual plots of the dependent variable against time were too cluttered to show any trends in the data. For this reason, the data for each variable (eg, bracket and arch) were smoothed using a restricted cubic spline, which allowed for irregularly spaced data, and the resulting predicted smoothed values were plotted against time. These plots were an exploratory analysis to show trends and did not imply a formal relationship between the variables. The splines have increased errors with increasing time because of the reduction in the amount of data still present.
Because the data were recorded at irregular time intervals, the appropriate analysis involved mixed models rather than standard repeated-measures analysis of variance (ANOVA), which would require each patient visit to be at the same time. This would mean the use of the incorrect nominal time. The mixed-models approach also allowed for the fact that measurements on arch (jaw) were clustered in each patient. Stata module “xtmixed” was used with restricted maximum likelihood estimation, and effects were compared using margins in conjunction with Sidak’s adjustment for multiple comparisons. Two participants dropped out of this trial. However, their data until dropout were included in the statistical analysis because of the use of the linear mixed-model analysis instead of conventional ANOVA.
Results
The demographic data on Frankfort mandibular plane angle, sex, age, and initial Little’s index value for the bracket groups are shown in Table I . Summary statistics for the time to initial alignment are shown in Table II . The repeatability data for Little’s index and space closure were analyzed using Lin’s concordance correlation coefficient, ρ c , which is a product of the Pearson correlation coefficient, r , a measure of precision; and the bias correction factor, Cb , a measure of accuracy. For both measures, the accuracy over the 2 time periods was Cb = 1.00. For Little’s index, ρ c = 0.996 [0.989, 0.992]; for extraction space measurements, ρc = 0.999 [0.998, 0.999]. Patient flow through the trial is illustrated in Figure 1 . The recruitment span was 2006 to 2010, with the last patient debonded in 2011.
| Damon 3MX | In-Ovation R | Omni | |
|---|---|---|---|
| Male | |||
| n | 17 | 12 | 8 |
| Age (y) | 14.3 (1.1) | 14.1 (1.5) | 14.3 (0.9) |
| Female | |||
| n | 25 | 26 | 12 |
| Age (y) | 14.2 (1.3) | 13.8 (1.4) | 13.2 (1.5) |
| Frankfort mandibular plane angle | |||
| Low | 4 | 4 | 11 |
| Average | 27 | 25 | 9 |
| High | 11 | 9 | 5 |
| Little’s index (mm) | |||
| Maxilla | 11.42 | 12.17 | 10.59 |
| (1.89-25.82) | (2.66-23.52) | (3.28-19.98) | |
| Mandible | 8.80 | 8.17 | 6.75 |
| (4.01-19.75) | (2.60-14.51) | (2.15-15.55) |
| Bracket | n | Mean time (d) | SD (d) | Max time (d) |
|---|---|---|---|---|
| Damon 3MX | 41 | 422 | 124 | 749 |
| In-Ovation R | 37 | 399 | 107 | 664 |
| Omni | 20 | 251 | 107 | 470 |
| Total | 98 | 379 | 131 | 749 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


