Introduction
Cervical vertebral column morphology and head posture were examined and related to craniofacial morphology in preorthodontic children and adolescents with anterior open bite.
Methods
One hundred eleven patients (ages, 6-18 years) with an anterior open bite of more than 0 mm were divided into 2 groups of skeletal or dentoalveolar open bite. The skeletal open-bite group comprised 38 subjects (19 girls, 19 boys). The dentoalveolar open-bite group comprised 73 subjects (43 girls, 30 boys). Visual assessment of the cervical column and measurements of craniofacial morphology and head posture were made on profile radiographs.
Results
Deviations in the cervical vertebral column morphology occurred in 23.7% of the subjects in the skeletal open-bite group and in 19.2% in the dentoalveolar open-bite group, but the difference was not significant. Head posture was significantly more extended in the skeletal open-bite group compared with the dentoalveolar open-bite group (craniovertical angle [Mx/VER], P <0.05; craniocervical angles [Mx/OPT, Mx/CVT], P <0.01. Only head posture was associated with craniofacial morphology: extended posture was associated with a large cranial base angle ( P <0.01, P <0.001), large vertical craniofacial dimensions ( P <0.05; P <0.01; P <0.001), and retrognathia of the jaws ( P <0.001).
Conclusions
Cervical column morphology is described for the first time in children and adolescents with open bite. No significant differences in the cervical vertebral column’s morphologic deviations were found between the skeletal and the dentoalveolar open-bite groups. Significant differences were found in head posture between the groups and with regard to associations with craniofacial dimensions. This might indicate a respiratory etiologic component in children with anterior open bite.
Deviations of cervical column morphology are observed in healthy subjects with neutral occlusion and normal craniofacial morphology as well as in patients with craniofacial syndromes, deviating craniofacial morphology, and severe malocclusion traits. A recent study found that fusion between cervical vertebrae C2 and C3 occurs in 14.3% of healthy subjects. Fusions of the upper cervical column within that range are thus considered normal.
Previous studies have found an association between deviant morphology of the upper cervical vertebrae and cleft lip and palate. Recently, an association has also been suggested between deviant morphology of the upper cervical vertebrae not only in patients with condylar hypoplasia, but also in adult orthodontic surgical patients with severe skeletal malocclusion traits. Deviations occurred significantly more often in these patients with severe skeletal malocclusion than in the control group. Furthermore, an association has been shown between cervical vertebral column morphology and horizontal maxillary overjet more than 6 mm in children; deviations occurred significantly more often in children with mandibular retrusion compared with children with maxillary dentoalveolar protrusion.
Previous studies of adults and children have found that fusion between C2 and C3 and occipitalization (eg, fusion between the first cervical vertebral unit and the occipital bone) are significantly associated with posture of the head and neck. These studies showed that the cervical vertebral column was more curved, the inclination of the upper cervical spine was more backward in adults with fusion, and the head in relation to the cervical vertebral column was more extended in children with occipitalization.
Furthermore, it has previously been demonstrated that the posture of the head and neck is associated with craniofacial morphology. It was found that an extended head posture in relation to the cervical vertebral column was associated with increased vertical craniofacial dimensions and reduced sagittal jaw dimensions.
The above-mentioned studies suggest that morphologic deviations of the upper cervical vertebrae are associated with craniofacial morphology, posture of the head and neck, and skeletal malocclusion traits. Furthermore, an association has been shown between head posture and craniofacial morphology, especially in the vertical dimension.
Accordingly, it is relevant to focus on similar associations among cervical column morphology, craniofacial morphology, and head posture in preorthodontic children and adolescents. Seemingly, no studies have yet been performed on cervical column morphology and head posture in relation to craniofacial morphology in preorthodontic children and adolescents with anterior open bite. Furthermore, new results have indicated that 2-dimensional lateral cephalograms (already available in connection with treatment planning, for example) are sufficient for identifying morphologic deviations in the cervical vertebral column.
The aims of this study were (1) to compare morphology of the cervical column and head posture in a group of children with skeletal anterior open bite (skeletal open-bite group) with a group of children with dentoalveolar anterior open bite (dentoalveolar open-bite group) and (2) to analyze the morphology of the cervical column and head posture in relation to the craniofacial morphology in both groups combined.
Material and methods
One hundred eleven profile radiographs were systematically selected according to the inclusion criteria (mentioned below) from patients registered between 1988 and 1997 at the orthodontic clinic, Municipal Dental Service of Farum, Denmark, and divided into 2 groups according to the type of anterior open bite: skeletal open bite or dentoalveolar open bite.
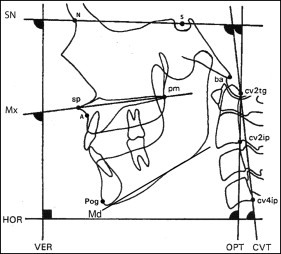
The skeletal open-bite group comprised 38 patients: 19 girls (ages, 6-16 years; mean, 9.8 years) and 19 boys (ages, 7-18 years; mean, 9.4 years). The inclusion criteria were (1) no prior orthodontic treatment, (2) skeletal open bite of more than 0 mm (vertical jaw relationship [ Fig 1 ] larger than 1 SD [Mx/Md >31°] according to the standards described by Björk and assessed by lateral radiographs of each subject), (3) no craniofacial syndromes or systemic muscle or joint disorders, and (4) a profile radiograph taken before orthodontic treatment with the 5 first cervical vertebral units visible. The sagittal jaw relationship (A-N-Pog, Fig 1 ) ranged between 0.0° and 14.5° (mean, 4.7°), the horizontal overjet was between 0 and 10.5 mm (mean, 4.8 mm), the vertical jaw relationship (Mx/Md, Fig 1 ) was between 31.5° and 40.0° (mean, 34.3°), and the vertical overbite was between −6.6 and 0 mm (mean, −1.4 mm) ( Table I ).
| Variables | Skeletal (n = 38 ) | Dentoalveolar (n = 73) | Group | Sex | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P | P | |
| Cranial base angle (°) | ||||||
| N-S-Ba | 131.6 | 5.2 | 131.8 | 5.9 | NS | * |
| Sagittal dimensions (°) | ||||||
| A-N-Pog | 4.7 | 3.2 | 3.9 | 2.3 | NS | NS |
| S-N-A | 79.3 | 6.2 | 80.6 | 3.9 | NS | NS |
| S-N-Pog | 75.9 | 3.3 | 77.1 | 3.6 | NS | NS |
| Vertical dimensions (°) | ||||||
| Mx-Md | 34.3 | 2.2 | 27.2 | 2.8 | ‡ | NS |
| SN-Mx | 6.0 | 3.8 | 7.8 | 3.2 | * | NS |
| SN-Md | 39.6 | 3.5 | 34.6 | 4.0 | ‡ | NS |
| Incisor relations (mm) | ||||||
| Overjet | 4.8 | 2.9 | 5.1 | 3.5 | NS | NS |
| Overbite | −1.4 | 1.6 | −1.1 | 1.0 | NS | NS |
| Head posture (°) | ||||||
| SN/VER | 100.9 | 5.2 | 101.0 | 4.6 | NS | NS |
| Mx/VER | 95.4 | 4.5 | 93.5 | 4.3 | * | * |
| SN/OPT | 98.4 | 7.9 | 96.5 | 7.5 | NS | * |
| Mx/OPT | 93.1 | 7.5 | 88.7 | 7.2 | † | * |
| SN/CVT | 102.6 | 7.8 | 100.8 | 7.3 | NS | † |
| Mx/CVT | 97.5 | 6.8 | 93.6 | 7.0 | † | † |
| OPT/HOR | 92.5 | 6.9 | 94.5 | 7.8 | NS | NS |
| CVT/HOR | 88.1 | 5.8 | 90.1 | 7.0 | NS | NS |
| OPT/CVT | 4.4 | 2.8 | 4.7 | 3.0 | NS | NS |
The dentolveolar open-bite group comprised 73 subjects: 43 girls (ages, 7-14 years; mean, 6.4 years), and 30 boys (ages, 7-16 years; mean, 9.5 years). The inclusion criteria were (1) no prior orthodontic treatment, (2) dentoalveolar open bite of more than 0 mm (vertical jaw relationship within 1 SD [Mx/Md >15° and <31°] according to the standards described by Björk and assessed by lateral radiographs of each subject), (3) no craniofacial syndromes or systemic muscle or joint disorders, and (4) a profile radiograph taken before orthodontic treatment with the 5 first cervical vertebral units visible. The sagittal jaw relationship (A-N-Pog, Fig 1 ) ranged between 0.0° and 11.5° (mean, 3.9°), the horizontal overjet was between −3.0 and 13.0 mm (mean, 5.1 mm), the vertical jaw relationship (Mx/Md, Fig 1 ) was between 20.5° and 31° (mean, 27.2°), and the vertical overbite was between −4.0 and 0.0 mm (mean, −1.1 mm) ( Table I ).
The differences in mean values for craniofacial dimensions and head posture between the 2 groups and sexes are presented in Table I .
The morphology of the cervical column was evaluated by visual inspection of the first 5 cervical vertebral units as they are normally seen on a standardized lateral skull radiograph. Characteristics of the cervical column were classified according to the study of Sandham and divided into 2 categories.
- 1.
Posterior arch deficiency, defined as partial cleft and dehiscence. Partial cleft is defined as failure to fuse of the posterior part of the neural arch ( Fig 2 ), and dehiscence is defined as failure to develop of a part of a vertebral unit.
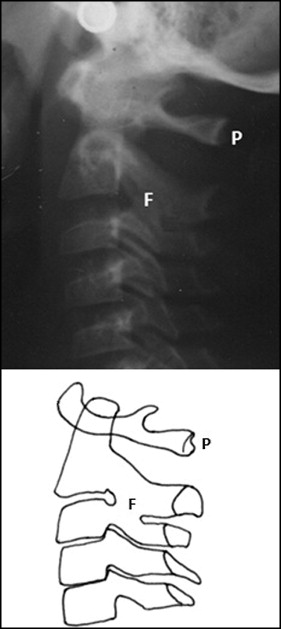
Fig 2 A profile radiograph and a graphic drawing illustrating partial cleft of the posterior part of the neural arch of atlas ( P ) and fusion of the second and third cervical vertebrae at the articulation facet ( F ). - 2.
Fusion anomalies, categorized as fusion, block fusion, and occipitalization. Fusion is defined as fusion of 1 unit with another at the vertebral bodies, articulation facets, neural arch, or transverse processes ( Fig 2 ). Occipitalization is defined as assimilation, either partially or completely, of the atlas with the occipital bone. Block fusion is defined as fusion of more than 2 units at the vertebral bodies, articulation facets, neural arch, or transverse processes.
Only deviations confirmed on the second profile radiograph or at a later date were accepted as morphologic deviations of the cervical vertebral column. If there was any doubt regarding the assessment of the cervical vertebral column, it was registered as having “no morphological deviations.” All assessments were checked by an author (L.S.).
For the craniofacial dimensions, the profile radiographs were taken with the teeth in occlusion and in the standardized head posture, the mirror position, as described by Siersbæk-Nielsen and Solow. The radiographs were taken in a cephalostat with a film-to-focus distance of 180 cm and a film-to-median plane distance of 10 cm. No correction was made for the constant linear enlargement of 5.6%. The reference points were marked and measured by hand on the profile radiographs using a protractor ( Fig 1 ). All points were checked by an author (L.S.). Eighteen variables representing the cranial base angle, the vertical and sagittal craniofacial dimensions, and head posture were calculated. A list of the variables is presented in Table I .
The reliability of the variables describing the cranial base, the vertical and sagittal craniofacial dimensions, and head posture was assessed by remeasuring 25 lateral radiographs selected at random from the previously evaluated radiographs. The radiographs were marked and measured again, and we found no significant differences with paired t tests between the 2 sets of recordings. The method errors calculated by Dahlberg’s formula ranged from 0.00° to 2.40°, and the Houston reliability coefficient ranged from 0.84 to 1.00. The reliability was within the same range as traditional film-based radiographs.
The reliability of the visual assessment of the morphologic characteristics of the cervical vertebral units has been reported previously (k = 0.82).
Statistical methods
Regarding the craniofacial dimensions, the effect of age was assessed by linear regression analysis and for morphologic characteristics of the cervical column by logistic regression analysis. Differences in the means of the craniofacial dimensions between the sexes and between the groups were assessed by unpaired t tests. Differences in the occurrence of the morphologic characteristics of the cervical column between the sexes and between the groups were assessed by the Fisher exact test. Associations between the morphology of the cervical column and each craniofacial dimension were expressed in terms of Nagelkerke logistic regression correlation coefficients (R) and tested for the possible effects of age and sex by multiple logistic regression analyses. Associations between head posture and craniofacial morphology and the possible effects of age and sex were tested by multiple linear regression analyses. The results from the tests were considered significant at P values less than 0.05. The statistical analyses were performed using SPSS software (version 20.00; SPSS, Chicago, Ill).
Results
We studied the morphology of the cervical column. In the skeletal open-bite group, 7.9% of the subjects had fusion between the second (C2) and third (C3) cervical vertebrae, and 2.6% had block fusion between C2, C3, and C4. Also, 13.2% had a partial cleft of the posterior part of the neural arch of the atlas. Dehiscence and occipitalization did not occur ( Table II ). No statistical sex or age differences were found in the occurrences of the morphologic characteristics of the cervical column.
| Variable | Skeletal open-bite group | Dentoalveolar open-bite group | P | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Total column deviations | 9 | 23.7 | 14 | 19.2 | NS |
| Fusion anomalies | |||||
| Fusion of C2 and C3 | 3 | 7.9 | 8 | 11.0 | NS |
| Occipitalization | 0 | 0 | 0 | 0 | NS |
| Block fusion | 1 | 2.6 | 0 | 0 | NS |
| Posterior arch deficiency | |||||
| Partial cleft | 5 | 13.2 | 4 | 5.5 | NS |
| Dehiscence | 0 | 0 | 0 | 0 | NS |
| More than 1 deviation | 0 | 0 | 2 | 2.7 | NS |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


