History of the Procedure
Lorenz Heister first identified the buccal fat pad (BFP) in 1727. He thought it was glandular in nature and identified it as the “glandula molaris” in his Compendium Anatomicum. In 1801, Marie-Francois-Xavier Bichat was the first to provide the anatomic description of the BFP as a fatty tissue. Since then, it has been referred to in the medical literature by different names, including the boule de Bichat, masticatory fat pad, sucking pad, and sucking cushion.
The BFP had limited clinical use for many years. It was considered a surgical nuisance because it could be accidentally encountered during various surgical procedures in the oral cavity and pterygomaxillary space. Its use increased after Egyedi described methods of using the BFP for closing oronasal and oroantral communications and as a versatile pedicle graft for closing postsurgical maxillary defects. Tideman et al. described its detailed anatomy and vascular supply and the appropriate operative technique. Rapidis et al., Hao, Dean et al., Toshihiro et al., and Singh et al. used pedicle BFP for reconstruction of small and medium-sized postsurgical oral defects of malignant lesions.
History of the Procedure
Lorenz Heister first identified the buccal fat pad (BFP) in 1727. He thought it was glandular in nature and identified it as the “glandula molaris” in his Compendium Anatomicum. In 1801, Marie-Francois-Xavier Bichat was the first to provide the anatomic description of the BFP as a fatty tissue. Since then, it has been referred to in the medical literature by different names, including the boule de Bichat, masticatory fat pad, sucking pad, and sucking cushion.
The BFP had limited clinical use for many years. It was considered a surgical nuisance because it could be accidentally encountered during various surgical procedures in the oral cavity and pterygomaxillary space. Its use increased after Egyedi described methods of using the BFP for closing oronasal and oroantral communications and as a versatile pedicle graft for closing postsurgical maxillary defects. Tideman et al. described its detailed anatomy and vascular supply and the appropriate operative technique. Rapidis et al., Hao, Dean et al., Toshihiro et al., and Singh et al. used pedicle BFP for reconstruction of small and medium-sized postsurgical oral defects of malignant lesions.
Indications for the Use of the Procedure
Within the past decade, many reports have described the use of the buccal fat pad as a flap for oral reconstruction after tumor removal or for other oral lesions. The BFP has also been successfully used as an unlined pedicle graft for maxillary defects, such as defects in the alveolar crest, maxilla, hard and soft palate, cleft, retromolar region of the mandible, and vestibular sulcus. In addition, the BFP has often been used to repair palatal defects.
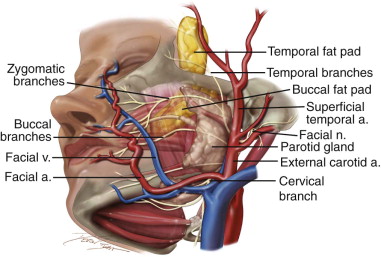
Surgery involving the hard palate frequently can leave oroantral or oronasal defects, resulting in considerable difficulty in speech and deglutition. Because of its close proximity to oral defects, the BFP can be used for reconstruction. It can also be used to effectively reconstruct small to medium-sized posterior maxillary alveolar defects. Thus, the buccal fat pad can be used to cover defects resulting from traumatic injury or malignant tumors of the soft tissue of the oral cavity. Pedicle fat pad grafts are advantageous because they reduce the invasiveness and duration of the operation, and buccal fat pads used to reconstruct defects have been shown to reduce pain and operative trauma. In addition, the rich blood circulation to the soft tissue promotes the healing of nearby structures. The grafted fat pad also functions as a site for granulation (thus limiting scar contraction) and can physically close dead space of a defective area. Furthermore, the buccal fat pad has strong antiinfection and reconstruction advantages, with little necrosis or reabsorption ( Figure 107-1 ).
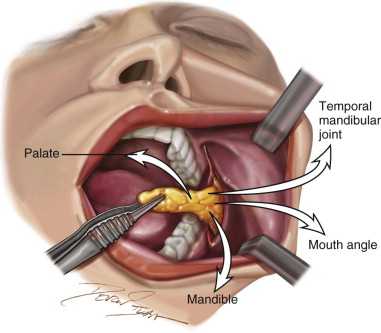
Clinical Uses of the Buccal Fat Pad Flap ( Figure 107-2 )
- 1.
Closure of oral antral communication (OAC)/oral antral fistula (OAF)
- 2.
Reconstruction of postexcision defect
- 3.
Closure of mucosal defects
- 4.
Treatment of oral subcutaneous fibrosis
- 5.
Repair of primary cleft
- 6.
Reconstruction of the temporomandibular joint
- 7.
Membrane in sinus floor augmentation
- 8.
Coverage of severe gingival recession defect
- 9.
Closure of anterior and middle skull base defects
- 10.
Treatment of osteoradionecrosis
- 11.
Coverage of zygomatic implants (extrasinus technique)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


