Introduction
The purpose of this study was to evaluate the biologic response of dentoalveolar bone to archwire expansion with light-to-moderate continuous forces.
Methods
With a split-mouth experimental design, the maxillary right second premolars of 7 adult male dogs were expanded for 9 weeks using passive self-ligating brackets (Damon Q; Ormco, Orange, Calif) and 2 sequential archwires (0.016 × 0.022-in copper-nickel-titanium alloy, followed by 0.019 × 0.025-in copper-nickel-titanium alloy). Intraoral and radiographic measurements were made to evaluate tooth movements and tipping associated with expansion; archwire forces were measured using a force gauge. Microcomputed tomography was used to compare buccal bone height, total tooth height, total root height, and buccal bone thickness. Bone formation was evaluated histologically using tetracycline and calcein fluorescent labels and hematoxylin and eosin stains.
Results
Buccal expansion was produced by forces between 73 and 178 g. Compared with the control side, which showed no tooth movement, the experimental second premolars were expanded by 3.5 ± 0.9 mm and tipped by 15.8°. Buccal bone thickness was significantly thinner (about 0.2 mm) in the coronal aspects and significantly thicker (about 0.9 mm) in the apical aspects over the mesial roots. The tipping and expansion significantly ( P <0.05) reduced buccal bone height (ie, caused dehiscences) at the mesial (about 2.9 mm) and distal (about 1.2 mm) roots. Bony apposition occurred on the trailing edges of tooth movement and on the leading edges of the second premolar apices. The axial microcomputed tomography slices indicated, and the bone histomorphometry and histology demonstrated, newly laid-down bone on the periosteal side of the buccal cortical surfaces. Ordered osteoblast aggregation was also evident on the periosteal surfaces of buccal bone, just cervical to the apparent center of rotation of the tooth. Tooth and root heights showed no significant differences between the experimental and control second premolars.
Conclusions
Buccal expansion with light-to-moderate continuous forces produced 3.5 mm of tooth movement, uncontrolled tipping, and bone dehiscence, but no root resorption. Bone formation on the periosteal surfaces of cortical bone indicates that apposition is possible on the leading edge of tooth movements.
A tooth size-arch length deficiency is a common problem faced by clinical orthodontists. This can be treated by reducing tooth size or by increasing space in the arch. To gain space and address transverse maxillary deficiencies, patients are often treated with archwire expansion. Unfortunately, root resorption is associated with dental expansion. Moreover, the palatal and buccal cortical plates can inhibit tooth movements before root resorption occurs. Although expansion has been purported to be possible without causing excessive tipping, most studies have reported tipping of posterior teeth from 7° to 13.5°. Tipping has been shown to cause dehiscences of buccal bone and root resorption.
Although it has been claimed that improved alveolar bone formation occurs, the effects of archwire expansion on the alveolar bone surrounding the teeth remain largely unknown. Can a tooth be expanded beyond the outer boundary of the buccal cortex? Does dental tipping cause significant dehiscence formation? Can dental expansion with light continuous forces create bone lateral to the tooth?
To address these questions, the aims of this project were to (1) evaluate the movements of the maxillary second premolars expanded with light-to-moderate continuous forces, (2) determine whether a multi-rooted premolar can be moved buccally through the maxillary cortex, and (3) evaluate the adaptation of bone when the teeth are expanded.
Material and methods
Seven male, periodontally healthy, mixed-breed dogs, each weighing 55 to 65 lbs and between 1 and 2 years of age (skeletally young adults), were used in this experiment. Previous split-mouth designs have shown significant differences in tooth movement with similar numbers of animals. The housing, care, and experimental protocol were approved by the Institutional Animal Care and Use Committee at Texas A&M University, Baylor College of Dentistry, Dallas, Tex.
The animals received a dental prophylaxis with an ultrasonic scaler with 0.2% chlorhexidine gluconate mouth rinse. Alginate impressions were made, and models were poured with dental stone. The maxillary right canines, second premolars, and fourth premolars, along with the control left second premolars, were banded. Orthodontic band material (Dentaurum, Ispringen, Germany) was custom formed, welded, and soldered to fit each tooth. Brackets (0.022 in) were welded to all 3 bands on the experimental right side; no brackets were welded to the control left second premolar bands. The canine bracket (3M Unitek, Monrovia, Calif) had 0° offset, 0° torque, and a 0.051-in headgear tube. The second premolar bracket (Damon Q; Ormco, Orange, Calif) had 0° offset and −11° torque. The fourth premolar bracket (3M Unitek) had 10° offset, −14° torque, and a 0.045-in headgear tube. The bands were perforated and microetched on the inner surface to increase retention of the bonding material.
The animals were sedated with ketamine (2.2 mg per kilogram intramuscularly) and xylazine (0.22 mg per kilogram intramuscularly) followed by intubation and delivery of 1.5% isoflurane in oxygen at 1 liter per minute. A high-speed handpiece and a 30-fluted carbide bur were used to remove any residual plaque and roughen the tooth surfaces. To further increase bond retention, a 330 burr was used to place undercut grooves across all surfaces of the crowns. The teeth were etched with 37% phosphoric acid gel (Reliance Orthodontic Products, Itasca, Ill) for 30 seconds. All-Bond 3 primers A and B (Bisco, Richmond, British Columbia, Canada) were applied, thinned slightly, and light-cured. All-Bond 3 adhesive resin (Bisco) was then applied, thinned, and light cured. The bands were then filled with 3M Transbond XT bonding resin (3M Unitek) and seated; excess composite was removed, and the resin was light-cured.
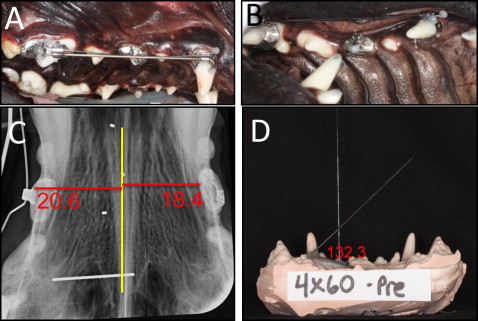
A 0.045-in stainless steel wire was bent and placed passively through the headgear tubes of the canines and the fourth premolars to protect the appliances buccally. A 0.016 × 0.022-in copper-nickel-titanium alloy wire (Ormco) was placed in the archwire slots of the canine and the fourth premolar brackets and then engaged into the second premolar. The ends of both wires were cinched, roughened, and bonded with composite for retention and comfort ( Fig 1 ). After 4 weeks, a 0.019 × 0.025-in copper-nickel-titanium alloy wire was placed and maintained for 5 additional weeks. After 9 weeks, the wire was deformed (passive) to ensure that no additional expansive forces were placed on the experimental second premolars. Passive consolidation lasted for 3 weeks. Fluorochrome bone markers were injected intramuscularly (25 mg per milliliter given at 10 mg per kilogram) at weeks 4 (tetracycline), 7 (calcein), and 10 (tetracycline) to label new bone deposition around the second premolars.
Archwire forces and intraoral width measurements were taken every 2 weeks. The force from the archwire on the experimental second premolars was measured twice using a Correx tension gauge (Haag-Streit, Köniz, Switzerland) and averaged. Three intraoral measurements, including intercanine width, intersecond premolar width, and interfourth premolar width, were taken twice with a digital caliper (General Tools, New York, NY) and averaged. Small notches were drilled into the cusp tips to ensure replicable placement of the caliper tips.
Metallic implants were placed in the midpalatal suture at the level of the second premolars and used as the sagittal reference lines for the radiographic measurements. Two occlusal radiographs (size 4 digital film) were taken every 2 weeks using a custom template (a 20-mm stainless steel reference bar was embedded in the template for calibrating tooth movements) to standardize the film position. The radiographs were exported to Dolphin Imaging (version 11.0; Patterson Dental Supply, Chatsworth, Calif), traced, and assessed with a custom analysis. A midline reference plane was drawn through the implant that was in the middle of the suture down through the 20-mm reference bar using the other implants for orientation. The perpendicular distances from the midline reference plane to the experimental and control second premolars were measured twice on each radiograph and averaged. For the experimental teeth, the most medial aspect of the bracket was used; on the control side, which did not have a bracket, the most medial part of the band was used. Seven sets of measurements were made over the 12-week experimental period ( Table I ).
| Week | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 2 | 4 | 6 | 7 | 8 | 9 | 10 | 12 | |
| Records | T0 | T1 | T2 | T3 | T4 | T5 | T6 | ||
| Wires | .016 × .022-in CuNiTi | .016 × .022-in CuNiTi | .019 × .025-in CuNiTi | .019 × .025-in CuNiTi | .019 × .025-in CuNiTi | .019 × .025-in CuNiTi | Passive | Passive | Passive |
| Bone markers | Tetracycline | Calcein | Tetracycline | ||||||
The last set of records included postexperiment alginate impressions from which the final casts were poured. To assess tipping, custom templates were fabricated with Triad acrylic (Dentsply International, York, Pa). One template was made for the stable palatal rugae and adjacent first and third premolars; another template was made for the experimental second premolars. Each template had a 0.036-in stainless steel wire bonded to it and extending from it. With both templates seated, the wires created an angle; tipping measurements were calculated from standardized photographs as the difference in the angles created before and after expansion. Tipping was measured twice and averaged.
After the dogs were sacrificed, the maxillae were disarticulated and sectioned to produce blocks of experimental and control bone that included the first, second, and third premolars. The blocks of bone were immediately stored in 20% ethanol. The blocks were oriented vertically, loaded into the Micro-CT 35 scanner (ScanCo Medical, Bassersdorf, Switzerland), scanned at 37 μm, and analyzed using the Micro-CT software (version 6.0; ScanCo Medical). To view the tooth movement and assess the bony adaptation around the roots, 2-dimensional slices were evaluated 4 mm apical to the furcation. Two-dimensional slices were also used to measure (1) buccal bone height, a measure of dehiscence, taken on each second premolar root from the most lingual aspect of buccal bone at the level of the apex to the beginning of the dehiscence; (2) total tooth height, a measure of root resorption, taken from the cusp tip to the apex of each root; (3) total root height, another measure of root resorption, measured at the middle of each root from the level of the furcation to the apices; and (4) buccal bone thickness, measured at both second premolar roots, from the most lingual to the most buccal aspects of buccal bone at the cervical (measured 4 mm apical to the level of the furcation), middle (measured exactly halfway between the cervical and apical measurements), and apical (measured at the tip of the apex) levels. All measurements were made twice, on different days, and averaged.
Both bone histomorphometry and traditional hematoxylin and eosin staining were performed. The 2 experimental second premolars that showed the most movements, with their respective controls, were evaluated either histomorphometrically or with traditional hematoxylin and eosin staining. The 2 second premolars that moved the least and the 2 premolars that moved an average distance were evaluated similarly. The 3 experimental hematoxylin and eosin specimens were sectioned using coronal orientations, and the 3 experimental histomorphometry specimens were sectioned using axial orientations. The remaining specimens were evaluated histomorphometrically with a coronal orientation ( Table II ).
| Dog | Side | Histology type | Orientation |
|---|---|---|---|
| A | Experimental | Histomorphometry | Axial |
| Control | Histomorphometry | Axial | |
| B | Experimental | H&E | Coronal |
| Control | NE | NE | |
| C | Experimental | H&E | Coronal |
| Control | H&E | Coronal | |
| D | Experimental | H&E | Coronal |
| Control | H&E | Coronal | |
| E | Experimental | Histomorphometry | Axial |
| Control | Histomorphometry | Axial | |
| F | Experimental | Histomorphometry | Axial |
| Control | Histomorphometry | Axial | |
| G | Experimental | Histomorphometry | Coronal |
| Control | NE | NE |
Statistical analysis
The data were analyzed statistically with SPSS software (SPSS, Chicago, Ill). Nonparametric Wilcoxon signed ranks tests were used to evaluate the differences between the experimental and control sides.
Results
Only 1 dog experienced weight loss, which was resolved after the first week. With the exception of that animal, the dogs’ food consumption, which was closely monitored throughout the experimental period, was normal.
Intersecond premolar widths increased by an average of 4.2 mm over the 63 days of active expansion; intercanine width decreased by 1.1 mm; and interfourth premolar width did not change. During the consolidation period (measurements 4-6), the intersecond premolar distance decreased slightly to 4.1 mm; intercanine width increased, resulting in 0.3 mm of total constriction; interfourth premolar distance width ended with 0.2 mm of expansion ( Fig 2 , A ). From the radiographic measurements, the experimental second premolar moved laterally by 3.4 mm during active expansion ( Fig 2 , B ). After consolidation, the premolar had been expanded by 3.5 mm. The control second premolar moved laterally by 0.4 mm after active expansion and by 0.3 mm after consolidation. At the end of consolidation, the experimental second premolars had tipped by an average of 15.8° (range, 9.8°-26.5°).
The force applied by the first wire (0.016 × 0.022 in) to the experimental second premolar was, on average, 150 g at the beginning of the experiment. After 4 weeks, the force had decreased to 73 g. At that same time, the second wire (0.019 × 0.025 in) was placed and produced an initial force of 179 g. At the end of active expansion, the average force of the second wire was 81 g. No force was applied during consolidation.
The 3-dimensional image reconstructions showed obvious dehiscences on the roots of the experimental second premolars ( Fig 3 ), especially on the mesial roots. The control second premolars showed no dehiscences. The 2-dimensional slices taken 4 mm apical to the furcation confirmed dehiscence on the mesial roots of all experimental second premolars and on the distal roots of 4 of the 7 dogs’ teeth ( Fig 4 ). Buccal bone heights at the experimental mesial roots (6.1 ± 1.9 mm) were significantly ( P = 0.028) shorter than were the control buccal bone heights (9.1 ± 1.1 mm). The buccal bone heights of the experimental and control distal roots were 6.0 ± 1.3 and 7.2 ± 1.0 mm, respectively, again resulting in a statistically significant difference ( P = 0.018) of 1.2 mm ( Fig 5 ).
Total tooth height, measured after consolidation, showed no significant differences between the roots of the experimental and control second premolars. Total root height also showed no significant difference between the experimental and control roots, indicating that no statistically significant apical root resorption occurred.
At the coronal level, buccal bone thickness of the mesial experimental roots was significantly ( P = 0.018) thinner (0.2 mm) than buccal bone thickness of the mesial roots on the control teeth ( Fig 6 ). At the apical level, buccal bone thickness was significantly ( P = 0.018) thicker (0.9 mm) on the mesial root of the experimental teeth than on the control teeth. No significant difference was found at the midlevel of the mesial root. On the distal root, no significant differences were found at any level, although the same pattern of differences was evident at the apical and coronal levels.


