Some nerve injuries require repair in order to regain sensory or motor function. Although this article focuses primarily on trigeminal nerve (TN) injuries and repairs, the facts presented may apply to any peripheral nerve repair. The primary indications for nerve repair or grafting are (1) an injury or continuity defect in a nerve, because of trauma, pathologic condition, surgery, or disease, that cannot regain normal function without surgical intervention and (2) loss of normal neurologic function, resulting in anesthesia, paresthesia, dysesthesia, or paralysis, that cannot be corrected by nonsurgical treatment. In some nerve injuries (eg, neurapraxia), the nerve regains sensory or motor function unless irreversible compression, neuroma (axonotmesis), or transection (neurotmesis) occurs. In more severe injuries, there may be a significant loss of nerve substance (continuity defect) or a section of nerve may need to be removed to expose normal nerve tissue in preparation for nerve repair. Thus, nerve repair and nerve grafting procedures may be required to provide continuity between the proximal and distal portions of the nerve.
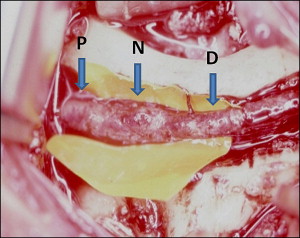
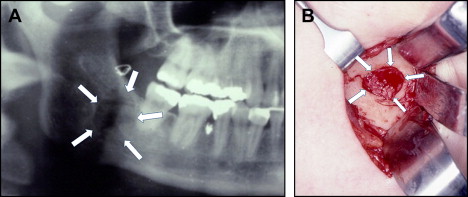
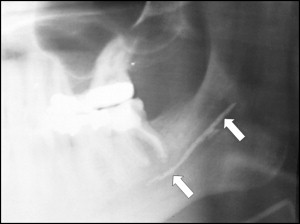
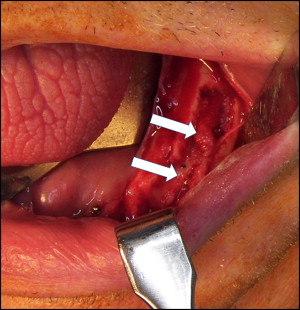
The 3 major branches of the TN that can be injured are the inferior alveolar nerve (IAN), lingual nerve (LN), and infraorbital nerve (ION). The most common types of injury to the IAN and LN are iatrogenic, related to the removal of impacted teeth ( Fig. 1 ), orthognathic surgery ( Fig. 2 ), periodontic surgery, endodontic surgery ( Fig. 3 ), dental implants ( Fig. 4 ), curettage of intrabony lesions, partial or total resection of the mandible or tongue in tumor removal, other surgical procedures, as well as trauma. Injuries to the ION are more commonly caused by trauma to the middle third of the face ( Fig. 5 A), partial or total maxillectomy and orbital exoneration during resection of benign or malignant tumors, or inadvertent nerve injury during maxillary and midface osteotomy. Nerve injuries that are more difficult to manage include severe stretch injuries and chemical injuries such as those that occur when alcohol, steroids, or other caustic agents are injected into or around nerves (see Fig. 3 ). The nature and extent of the nerve abnormality will influence the type and quality of repair.
Considerations for direct nerve repair
When surgical repair is required for a transected nerve or a nerve injury requiring excision, the best results, when conditions permit, are achieved with a direct nerve repair, without grafting. There are basically 3 types of nerve repair.
Perineural repair involves repairing the individual fascicles and placing sutures through the perineurium. Complications of this technique include trauma to the nerve in dissecting out each fascicle and fibrosis that develops because of the dissections and numerous sutures placed.
Group funicular repair involves repairing grouped fascicles with sutures placed through the intraneural epineurium, aligning groups of fascicles. The TN branches have nongrouped fascicles, so this technique is not applicable.
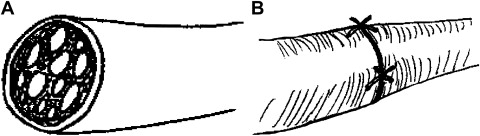
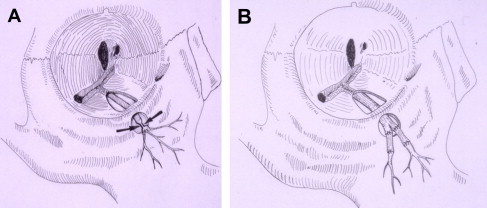
Epineural repair involves aligning the nerve ends and placing sutures through the epineurium only. Because the TN branches are polyfascicular (multiple different-sized fascicles) and nongrouped, the epineural technique is the most logical choice of repair method ( Fig. 6 ).