Introduction
Our objective was to assess the amounts of adhesive remnant and enamel damage when removing composite under conventional lighting and ultraviolet (UV) light.
Methods
Thirty-eight premolars were divided into 2 groups according to the lighting used for adhesive removal. A multifluted tungsten-carbide bur at low speed was used for this process in both groups. The UV group received conventional lighting associated with UV light, and the conventional group received conventional lighting only. The amounts of adhesive remnant were calculated using images of the teeth taken under UV light with software. Scanning electron microscopy images of epoxy adhesive replicas of the teeth made before bonding and after adhesive removal were graded according to the enamel damage index (EDI), and the difference between the final and initial EDI scores was used for assessment of the enamel damage. To detect differences between the groups, the Mann-Whitney test was used to analyze the data from the adhesive remnant index and the EDI.
Results
The conventional group had more adhesive left on the enamel ( P <0.001) than did the UV group. There was no difference between groups for the EDI ( P = 0.729).
Conclusions
UV lighting allows significantly more adhesive removal without increasing the damage caused to the enamel.
Highlights
- •
The use of UV light to assist the resin removal procedure was tested.
- •
With UV light, more resin is removed from enamel surfaces.
- •
The use of UV light did not cause more damage to enamel.
At the end of orthodontic treatment, the clinician needs to remove the adhesive left after debonding with as little damage as possible to the enamel. However, this extreme care during the process may prevent all adhesive from being removed; that in turn could cause 2 major problems. One is the possible creation of retentive areas that might favor biofilm buildup, subsequent decalcification, and carious lesions; the second problem involves pigmentation of adhesive remnants caused by aging, leading to patient dissatisfaction.
Even though the adhesive removal task appears simple and easy, excess bonding material is often overlooked because the orthodontic adhesive has a similar color to the enamel. Moreover, the use of filled adhesive sealants aimed at preventing white spot lesions further requires the material to blend in with the color of the enamel. The clinician must have confidence during adhesive removal that a clean, but damage-free enamel surface can be attained. However, to date, no damage-free adhesive removal technique has been described. Even though it is one of the safest methods for adhesive removal, the use of low-speed multifluted tungsten-carbide burs will still cause injuries with depths varying from 0.05 to 50 μm. Thus, it seems logical that an adhesive removal method that will not alter the adhesive color, but could render the removal process easier and possibly safer would be advantageous during the debonding process.
More recently, ultraviolet light (UV) fluorescent chemicals have been added to orthodontic adhesives, allowing UV light to be used as an aid to adhesive remnant removal. In addition, light-curing devices with UV light filters are already available on the market, allowing this alternative method to be clinically applied. Nevertheless, the use of this technology has not been tested scientifically; therefore, its effectiveness remains questionable.
Based on the potential of causing the least damage to dental enamel and the lack of orthodontic studies on the subject, the aim of this study was to assess whether the removal of adhesive with fluorescent properties under UV light is more effective and causes less damage to enamel than conventional lighting.
Material and methods
Due to a lack of similar studies in the literature and because the brackets were removed by a shear bond strength test, the sample size calculation was carried out with data from the literature on shear bond strength tests. A sample size of 18 teeth was found to be adequate using data from the literature. The number was determined with significance of 5% and power of 80%; moreover, to ensure that an appropriate sample was available if any unavoidable failure occurred, 20 specimens were used per group.
A total of 40 premolars with no brackets previously bonded and free of caries, fractures, and restorations were acquired from the tooth bank of the Faculdade de Odontologia de Araraquara (Universidade Estadual Paulista). The use of these teeth for this research was approved by the ethics and research project committee of the university, collected through donations, with consent from the patients, and after extractions for orthodontic or periodontal reasons. The teeth were stored in distilled water at 4°C for not longer than 3 months according to the International Organization for Standardization standard 11405:2014.
The teeth were vertically embedded in acrylic resin in polyvinyl chloride cylinders (diameter, 0.5 in; height, 3 cm) up to the cementoenamel junction. A metal square was used to align the surfaces of the teeth perpendicular to the bottom of the cylinder.
The surfaces of the premolars were cleaned and pumiced with an oil-free paste and a rubber cup for 15 seconds, washed, and completely air dried for 10 seconds with oil-free air and water. The buccal dental enamel was conditioned with 37% phosphoric acid for 30 seconds, washed, and completely dried for 10 seconds with oil-free air and water. The liquid adhesive was applied (Opal Seal; Opal Orthodontics, South Jordan, Utah) and light cured for 6 seconds with the VALO LED (Ultradent, South Jordan, Utah) on extra power. All premolars had 0.022-in slot brackets (Opal Orthodontics) bonded to them using the UV-sensitive composite Opal Bond MV (Opal Orthodontics). The brackets used had a bonding base with an average area of 11.045 mm 2 .
The specimens were maintained in distilled water at 37°C for 24 hours before the shear bond strength test, which showed adequate bond strength, ranging from 13.16 to 19.43 MPa. Since 1 tooth was fractured during the test, another was randomly removed from the sample to produce 2 equal groups.
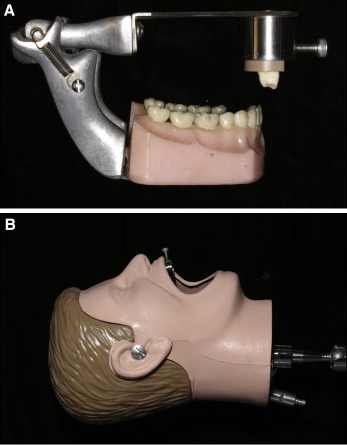
After debonding, the teeth were randomly divided into 2 groups of 19 according to the lighting to be used for removal of the adhesive remnants. The adhesive removal of 1 group was done under conventional lighting emitted by a dental chair unit, and the operator (L.F.A.) used a UV light-emitting diode flashlight to reveal the adhesive by fluorescence, whereas the other group received conventional lighting only. The procedure was performed with a 12-bladed tungsten-carbide bur (Orthometric, Marília, São Paulo, Brazil) in a low-speed hand piece. To make the procedure similar to that performed clinically, the teeth were adapted to a mannequin head for the removal procedure ( Fig 1 ).
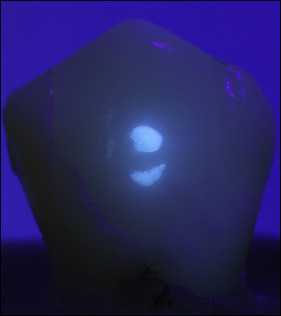
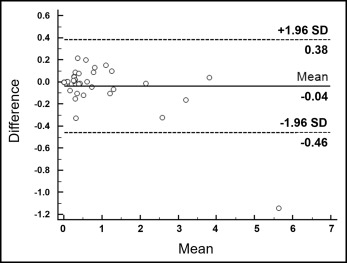
To assess the amount of adhesive remnant on the enamel surface, the teeth were photographed under a UV light filter adapted to a light-emitting diode (VALO, Ultradent) ( Fig 2 ) using a digital camera (EOS Rebel T3i; Canon, Tokyo, Japan) with a 90-mm macro lens, 1/60 shutter speed, F 8.0, and ISO 400. The photographs were scaled, and the area of adhesive remaining after the removal process was measured by Image J software (version 1.36; National Institutes of Health, Rockville, Md). Two measurements were taken by the same operator (L.F.A.) a week apart to evaluate the method error using Bland-Altman plots. Bias was 0.04, and the limits of agreement ranged from 0.38 to −0.46 mm 2 ( Fig 3 ). To reduce error, the average of the 2 measurements of each specimen was for the statistical analyses.
Enamel damage was assessed using epoxy resin replicas (Epofix; Struers, Ballerup, Denmark), which were made by taking impressions of the specimens before bonding and after adhesive removal with light polyvinylsiloxane material (Zhermack, Badia Polesine, Italy).
The replicas were coated with gold and photographed by scanning electron microscopy (JEOL, Tokyo, Japan) under 20-times magnification. One calibrated and blinded operator (L.F.A.) graded the enamel damage of all the specimens before bonding and after adhesive removal in a random sequence and assigning each photograph a score according to the Enamel Damage Index (EDI; Table I ). The after-adhesive-removal score ( Fig 4 , A ) was subtracted from the before-bonding score ( Fig 4 , B ) for comparison of the groups. Intraoperator error was determined by repeating measurements after 7 days and analyzing these by a weighted kappa test; this resulted in a value of 0.9.
| Score | Surface characteristics |
|---|---|
| 0 | Smooth surface without scratches, visible perikymata ∗ |
| 1 | Acceptable surface with fine scratches spread |
| 2 | Rough surface with several rough scratches or visible minor grooves |
| 3 | Surface with rough scratches, large grooves, and enamel damage visible with the naked eye |
∗ Perikymata are transverse wavy ridges that correspond to the incremental lines of Retzius.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


