I agree with Dr Kokich’s editorial in the September 2013 issue of the AJO-DO , urging us to join the orthodontic practice-based research network and the higher priority for the publication of clinical studies that are performed in-vivo. In-vitro studies are inarguably a primary understanding point in research. For example, the interactions of biomaterials applied extensively in orthodontics, such as bonding resins, nickel-titanium archwires, and elastomeric chains, have a highly applicable clinical value; however, they must carry the caveat that results from in-vitro and animal investigations do not always have a 1:1 relationship in humans.
The in-vitro discovery of penicillin mold for bacteria cytotoxicity has saved billions of lives and is an excellent example that justifies the consideration for upward positioning of in-vitro investigations in the evidence hierarchy above expert opinions, ideas, and editorials. This agrees with Dr Kokich that the lowest quality of evidence consists of expert opinion, and hence the necessary first building blocks of in-vitro and animal studies should hold a higher position than expert opinions in the evidence pyramid.
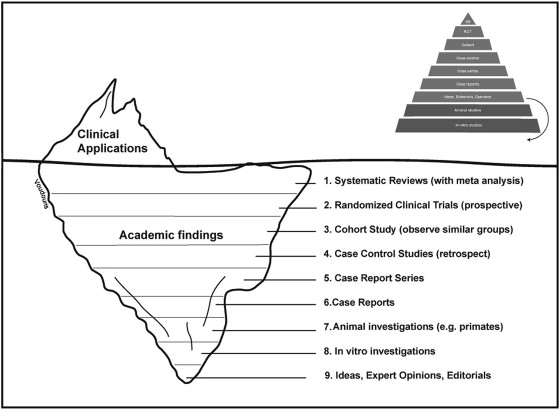
Actual clinical application is not represented at all in the older evidence pyramid diagram used in medicine. Thereby, we propose an “evidence iceberg” as a more realistic and complete representation of the hierarchy of investigations to now include the clinical application in orthodontics. Studies of highest relevance correspond to the largest and widest portion of the knowledge base, such as the systematic review (SR) with meta-analysis cross-comparing data, and the randomized controlled trial (RCT) ( Fig ). In contrast, the pyramid assigns the smallest areas to SRs and RCTs and the widest area to in-vitro studies. The evidence iceberg demonstrates a wide evidence-base of SRs and RCTs as a foundation, keeping afloat our viable clinical applications.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


