Armamentarium
|
History of the Procedure
The historical use for alveoplasty was to create a smooth and wide denture base. This shape provides optimal stability to the removable prosthesis. In 1853 Willard described contouring of the alveolar bone and contouring of the alveolar mucosa to obtain primary closure in preparation for denture placement. He stated that this should allow the patient to be restored sooner because the bone and tissue healed faster. In 1876 Beers described radical alveolectomy with cutting forceps. This was aggressive treatment, and clinicians reverted to being more conservative over the next 50 years. The procedure was not looked on favorably because the bone underwent a tremendous amount of bone loss after the surgery. The bone loss was thought to be due to the periosteal stripping and large flaps developed to provide access for the bone contouring surgery. In 1923 Molt recommended using models to plan the reshaping of the bone. His idea was to preserve bone and to maintain an appropriate vestibule.
In 1936 Dean described his technique to preserve the labial cortex and contoured intraradicular bone. This allowed him to compress the labial plate. No mucoperiosteal dissection leads to less pain, swelling, and bone resorption.
In 1976 Michael and Barsoum studied patients who had immediate denture placement and the amount of resorption associated with different surgical techniques, such as extraction without alveoplasty, extraction with labial alveolectomy, and extraction with intraseptal alveoplasty as described by Dean. The extractions alone had the least amount of bone loss; the labial alveoplasty had the most, even after 12 months.
The advent of implant dentistry has turned the table. Now, contemporary therapy focuses on maintaining as much bone as possible to facilitate implant placement. Moreover, augmenting the alveolus for rehabilitation purposes is fairly standard procedure.
History of the Procedure
The historical use for alveoplasty was to create a smooth and wide denture base. This shape provides optimal stability to the removable prosthesis. In 1853 Willard described contouring of the alveolar bone and contouring of the alveolar mucosa to obtain primary closure in preparation for denture placement. He stated that this should allow the patient to be restored sooner because the bone and tissue healed faster. In 1876 Beers described radical alveolectomy with cutting forceps. This was aggressive treatment, and clinicians reverted to being more conservative over the next 50 years. The procedure was not looked on favorably because the bone underwent a tremendous amount of bone loss after the surgery. The bone loss was thought to be due to the periosteal stripping and large flaps developed to provide access for the bone contouring surgery. In 1923 Molt recommended using models to plan the reshaping of the bone. His idea was to preserve bone and to maintain an appropriate vestibule.
In 1936 Dean described his technique to preserve the labial cortex and contoured intraradicular bone. This allowed him to compress the labial plate. No mucoperiosteal dissection leads to less pain, swelling, and bone resorption.
In 1976 Michael and Barsoum studied patients who had immediate denture placement and the amount of resorption associated with different surgical techniques, such as extraction without alveoplasty, extraction with labial alveolectomy, and extraction with intraseptal alveoplasty as described by Dean. The extractions alone had the least amount of bone loss; the labial alveoplasty had the most, even after 12 months.
The advent of implant dentistry has turned the table. Now, contemporary therapy focuses on maintaining as much bone as possible to facilitate implant placement. Moreover, augmenting the alveolus for rehabilitation purposes is fairly standard procedure.
Indications for the Use of the Procedure
Reshaping of the alveolar bone has multiple indications in maxillofacial surgery. All techniques used provide resurfacing or restructuring of the alveolar bone to provide a functional skeletal relationship. The indications for alveoplasty range from debulking procedures for pathologic conditions of the bone to recontouring the bone in preparation for prosthetic rehabilitation.
Simple plasty of the alveolar bone is defined as the reshaping of the alveolar bone during dental extraction surgery. If the alveolus has a sharp edge, the bone must be smoothed down to help with the healing process and prevent sequestra formation and pain.
The contouring of the alveolus after extractions also aids in prosthetic rehabilitation, whether with dental implants or dentures. Any sharp bone projections or edges under dentures create pain when the prosthesis compresses and rubs against them. The shape of the ridges for denture fabrication should maintain as much width and adequate height as possible to distribute forces properly. Undercuts must be addressed to allow for smooth placement of the prosthesis. The goals are to lose as little bone as possible after extraction, to maintain a wide alveolar ridge with the ideal U shape, and to get rid of undercuts that prevent smooth use and placement of a removable prosthesis.
With respect to dental implant rehabilitation, the reshaping of the alveolus is done to provide a stable base to place the dental implants and to create enough room for the prosthetic components necessary to restore the dentition. This may require removing some of the bone, which may be counterintuitive to the protocols for creating dentures.
Compression of the Alveolar Ridges
Compression is done after extractions when the labial, buccal, and lingual or palatal plates are expanded and create undercuts. These undercuts may interfere with denture comfort. This is simply done with finger pressure on the labial and palatal or buccal and lingual cortices to compress them together as tolerated by the tissues.
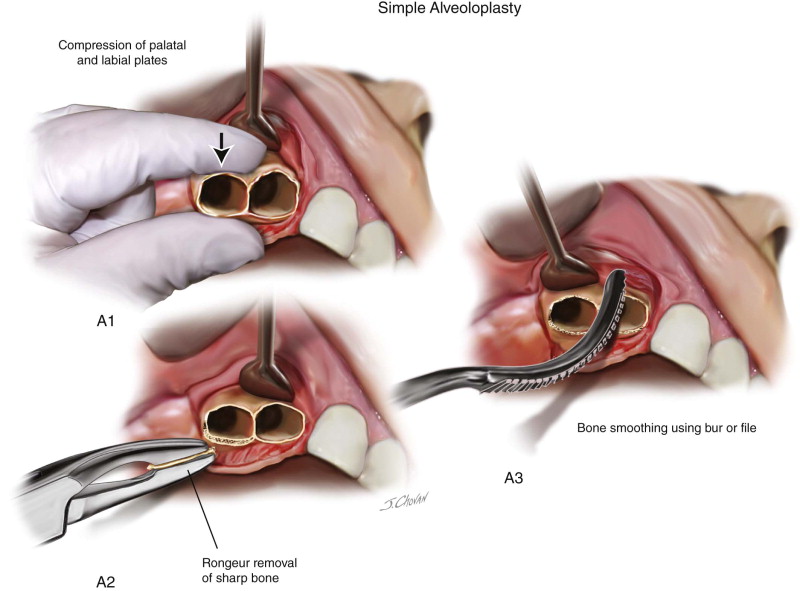
Technique: Simple Alveoloplasty
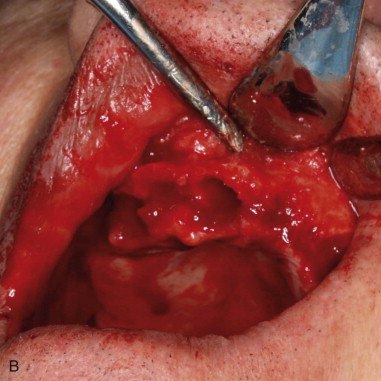
Simple alveoloplasty can be done in conjunction with or after extraction of teeth. It is typically intended to remove sharp edges, bony prominences, or undercuts in preparation for prosthetic rehabilitation. This is a surgical technique that should be as conservative as possible ( Figure 13-1, A and B ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


