Introduction
Historically, orthodontists have taken dental measurements on plaster models. Technological advances now allow orthodontists to take these measurements on digital models. In this study, we aimed to assess the accuracy, reproducibility, and time efficiency of dental measurements taken on 3 types of digital models.
Methods
emodels (GeoDigm, Falcon Heights, Minn), SureSmile models (OraMetrix, Richardson, Tex), and AnatoModels (Anatomage, San Jose, Calif) were made for 30 patients. Mesiodistal tooth-width measurements taken on these digital models were timed and compared with those on the corresponding plaster models, which were used as the gold standard. Accuracy and reproducibility were assessed using the Bland-Altman method. Differences in time efficiency were tested for statistical significance with 1-way analysis of variance.
Results
Measurements on SureSmile models were the most accurate, followed by those on emodels and AnatoModels. Measurements taken on SureSmile models were also the most reproducible. Measurements taken on SureSmile models and emodels were significantly faster than those taken on AnatoModels and plaster models.
Conclusions
Tooth-width measurements on digital models can be as accurate as, and might be more reproducible and significantly faster than, those taken on plaster models. Of the models studied, the SureSmile models provided the best combination of accuracy, reproducibility, and time efficiency of measurement.
Dental models provide a 3-dimensional view of a patient’s occlusion; this enables the clinician to evaluate the malocclusion in more detail than by a clinical examination. In orthodontics, measurements made on dental models are an integral part of the armamentarium used for diagnosis and treatment planning. In fact, dental models have been reported to be the major record used for orthodontic treatment planning.
Historically, orthodontists have used dental models made from plaster. With proper impression and pour-up techniques, these models provide an accurate representation of a patient’s dentition and surrounding structures. However, plaster models have limitations: they are at risk for breakage, chipping, or abrasion and create the need for storage rooms and their associated expenses. Technological advances have allowed orthodontists to perform measurements on digital models, which alleviate many of the obstacles encountered with plaster models. Digital models are not subject to physical damage or degradation, the digital file can be easily transferred to other clinicians or retrieved at multiple locations, and digital storage eliminates problems related to physical storage of traditional plaster models.
As a result of these advantages and their increasing affordability, more orthodontists are incorporating digital models into their practices. Currently, most digital models are made from alginate impressions, which are either scanned directly or poured in plaster and then scanned. With the increased use of cone-beam computed tomography (CBCT) in orthodontics, several companies have introduced another method of digital model fabrication. Sophisticated software algorithms now allow digital model fabrication from a patient’s CBCT scan; this eliminates the need for traditional impressions altogether.
Obviously, the potential advantages of digital models would be negated if the accuracy and efficiency of their measurements were not comparable with those taken on plaster models, the current gold standard with a long and proven history in orthodontics. Since many types of digital models are marketed to orthodontists today, these models need to be evaluated in the practice of evidence-based clinical orthodontics. The aims of this study were, therefore, to compare the accuracy, reproducibility, and time efficiency of dental measurements taken on 3 types of digital models with those taken on traditional plaster models, and to determine the model type that yields the best combination of accuracy, reproducibility, and time efficiency of measurement. Specifically, the digital models studied were emodels (GeoDigm, Falcon Heights, Minn), SureSmile models (OraMetrix, Richardson, Tex), and AnatoModels (Anatomage, San Jose, Calif).
Material and methods
The pretreatment models of 30 consecutive patients were used for this study. The patients had a variety of typical malocclusions and fully erupted permanent dentitions including incisors, canines, premolars, and first molars. Each patient had alginate impressions, a wax bite registration, and a CBCT scan taken as part of the diagnostic records. The CBCT scans were full field of view scans with a Next Generation i-CAT (Imaging Sciences International, Hatfield, Pa) at a voxel size of 0.3 mm 3 and a scan time of 8.9 seconds.
Plaster models were fabricated by pouring the alginate impressions in type II dental plaster (Modern Materials Orthodontic Plaster; Heraeus Kulzer, South Bend, Ind). emodels were then fabricated from these plaster models by GeoDigm. SureSmile models were fabricated by OraMetrix from CBCT scans of the plaster models taken with the Next Generation i-CAT at a voxel size of 0.2 mm 3 , a scan time of 26.9 seconds, and a wax-bite registration separating the maxillary and mandibular models to allow segmentation of the teeth. The plaster model, emodel, and SureSmile model of each patient were thus made from the same impressions and should have yielded identical measurements. AnatoModels were produced by Anatomage from the CBCT scan that had been taken as part of each patient’s diagnostic records. All models were deidentified before the study. The use of deidentified models had been approved by the institutional review board at the University of Minnesota.
Three calibrated operators (T.G., N.P., N.L.D.F.) measured the widths of the each tooth mesial to the second molars as the greatest mesiodistal diameter of their crowns as required for Bolton’s tooth-size analysis. In addition to their previous experience in the use of the types of dental models studied, the operators each measured 5 practice cases before data collection.
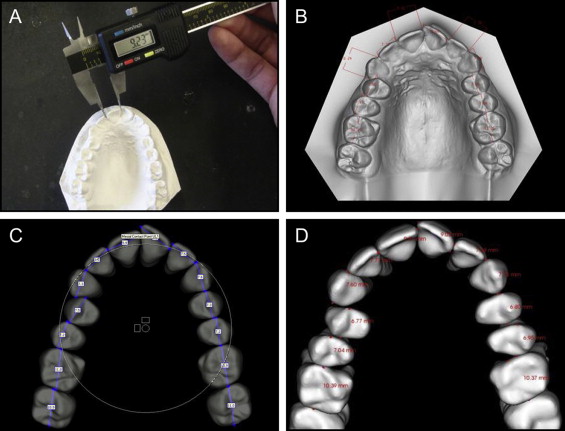
The measurements on the plaster models were taken manually using digital calipers (Ortho Organizers, Carlsbad, Calif), whereas those on the digital models were taken on a 22-in computer monitor (XPS; Dell, Round Rock, Tex) with landscape orientation at a screen resolution of 1680 × 1080 pixels using the software tools from the respective manufacturers ( Table I ). Measurements were taken to the nearest 0.01 mm on the plaster models, emodels, and AnatoModels, and to the nearest 0.1 mm on the SureSmile models because this is the smallest unit that can be measured with the SureSmile software. Examples of measurements with the various methods are shown in Figure 1 .
| Plaster model | emodel | SureSmile model | AnatoModel | |
|---|---|---|---|---|
| Model retrieval | Storage room | Server | Server | Server |
| Measuring tool | Digital calipers (calibrated between each set of models) | emodel software version 9.0 (GeoDigm) | SureSmile software version 5.9 (OraMetrix) | AnatoModel software version 5.0 (Anatomage) |
| Model manipulation | By hand | Virtual rotation and magnification | Virtual rotation and magnification | Virtual rotation and magnification |
| Software manipulation used to measure | NA | Analysis feature | Diagnostic model and new treatment simulation features | Occlusal layout feature with both arches visible |
| Selection of measuring points | By operator | By operator | By SureSmile technician; modified by operator | By operator |
| Time started | Models in front of operator | Models on computer screen | Models on computer screen | Models on computer screen |
| Time stopped | After recording all measurements | After completing measurements on computer | After completing measurements on computer | After completing measurements on computer |
| Measurements recorded | With pencil on a sheet of paper | On computer hard drive as an EMZ file | On SureSmile server | On computer hard drive as a JPEG file |
The 3 operators completed the measurements on all 30 models of 1 type before proceeding to the next model type. In each model type, the sequence in which the models were measured was randomized for each operator. Each set of measurements was timed to the nearest second using a digital stopwatch. For all models, the time was started when the models were in front of the operator, ready for analysis, and stopped when all measurements had been completed ( Table I ). After a washout period of 3 weeks, 6 cases were randomly selected from the original 30 and remeasured by all operators to assess within-rater repeatability.
Statistical analyses
Accuracy was assessed, separately for each type of digital model, as the degree of agreement between the measurements on the digital models and those on the corresponding plaster model using the method of Bland and Altman. To account for the correlation between tooth widths in a patient and to avoid underestimation of the variance, a mixed model with a random intercept term (for person) was used to obtain the variance estimates used in the Bland-Altman analysis. Bias was computed, separately for each type of digital model, as the average of the differences between the digital model measurements and the plaster model measurements for each tooth. Calculation of the limits of agreement during the Bland-Altman analysis provided limits that contained 95% of the differences for each type of digital model. When ranking the measurements on accuracy, both the bias and the variance were taken into account by calculating the mean squared error: mean squared error = bias 2 + variance.
Reproducibility, or between-rater reproducibility, was assessed as the degree of agreement between the measurements performed on replicate specimens by the 3 operators using the Bland-Altman method. The mean squared error was calculated to rank the measurements of reproducibility as detailed above.
Repeatability was assessed as the degree of agreement of measurements on the replicate specimens within each operator using the Bland-Altman method. Again, the mean squared error was calculated to rank the methods.
Time efficiency was assessed as the time required for measuring all tooth widths on the various model types. Mean values and standard deviations of the time required were calculated for each model type, and differences among the model types were tested for statistical significance using 1-way analysis of variance with the Tukey method as a post-hoc pairwise comparison after it had been confirmed that the data conformed to assumptions underlying parametric statistics (Kolmogorov-Smirnov test).
All statistical analyses were performed using R Statistical Software (version 2.9.2; R Foundation for Statistical Computing, Vienna, Austria), with P values of less than 0.05 considered statistically significant.
Results
Repeatability comparisons of individual tooth-width measurements are reported in Table II . On average, the measurements were repeatable to 0.05 mm for each type of dental model.
| Model | Bias (mm) | Lower limit of agreement (mm) | Upper limit of agreement (mm) | Limit of agreement interval width (mm) | Mean squared error |
|---|---|---|---|---|---|
| Plaster model | 0.048 | −0.304 | 0.400 | 0.704 | 0.035 |
| emodel | −0.028 | −0.410 | 0.355 | 0.765 | 0.039 |
| SureSmile model | −0.011 | −0.231 | 0.209 | 0.440 | 0.013 |
| AnatoModel | 0.006 | −0.487 | 0.500 | 0.987 | 0.063 |
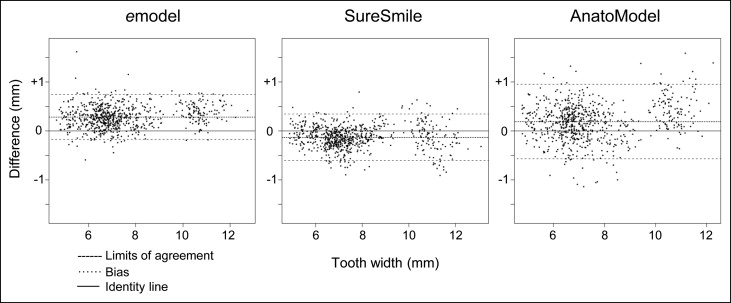
Accuracy comparisons of the tooth-width measurements are reported in Table III . The accuracy, as assessed by the mean squared error, was best for the measurements taken on the SureSmile models, followed by those on the emodels. The measurements on the AnatoModels were the least accurate. The Bland-Altman plots of tooth widths are shown in Figure 2 .
| Model | Bias (mm) | Lower limit of agreement (mm) | Upper limit of agreement (mm) | Limit of agreement interval width (mm) | Mean squared error |
|---|---|---|---|---|---|
| emodel | 0.285 | −0.176 | 0.746 | 0.922 | 0.134 |
| SureSmile model | −0.130 | −0.604 | 0.344 | 0.947 | 0.073 |
| AnatoModel | 0.191 | −0.57 | 0.952 | 1.521 | 0.181 |
Reproducibility comparisons for all operator combinations are reported in Table IV . Individual tooth-width measurements on the SureSmile models were consistently the most reproducible with the smallest mean squared errors between all 3 operator combinations. The measurements on the AnatoModels were consistently the third most reproducible, whereas those on the plaster models and the emodels interchanged from second to fourth most reproducible, depending on the operator combination.


