| SECTION III | ABNORMAL TOOTH MORPHOLOGY |
Crown malformations may be seen clinically upon visual inspection of the oral cavity.
1. Third Molar Malformations
Maxillary third molars have the most variable crown shape of all permanent teeth followed by mandibular thirds. These anomalies can range in shape from a small peg-shaped crown to a multicusped, malformed version of either the first or second molar.
2. Peg-Shaped Lateral Incisors
The most common anomaly in tooth shape in the anterior region of the permanent dentition is the peg-shaped (or cone-shaped) lateral incisor (Fig. 11-9) [which occur in 1% to 2% of the population].4 The tooth is somewhat conical in shape and broadest cervically and tapers toward the incisal to a blunt point. Several studies of identical twins seem to indicate that peg-shaped maxillary lateral incisor teeth may be a varied expression of the same genetic trait as missing maxillary lateral incisors.14,15 A most unusual occurrence is that of peg-shaped maxillary central incisors (Fig. 11-10). Recall that peg-shaped teeth develop from one lobe, instead of the four lobes, which would be normal for anterior teeth.

FIGURE 11-9. Peg-shaped maxillary lateral incisors. A. Incisal view on a plaster model. B. A peg-shaped lateral incisor seen in the mouth. C. Four extracted peg-shaped lateral incisors.

FIGURE 11-10. Peg-shaped maxillary central incisors, a very rare occurrence. A. Facial view. B. Incisal view showing both canines, one lateral incisor and the two peg-shaped central incisors.
3. Gemination or Twinning
Gemination or twinning results from the splitting (or twinning) of a single forming tooth. Since the tooth division is incomplete, the twinned crown appears doubled in width compared to a single tooth (Fig. 11-11) and notched. The single root is not split and has a common pulp canal. If the doubled tooth is counted as two teeth, the dental arch containing the geminated tooth will have an extra tooth beyond the normal number of teeth. Gemination occurs more frequently in the primary dentition than in the permanent dentition and most commonly in the region of the maxillary incisors and canines.3 [Gemination occurs in <1% of the population.] Note in Figure 11-12 that the wide, notched crowns of the anterior maxillary incisors of this Native American resemble teeth that have geminated.

FIGURE 11-11. Gemination (twinning). It appears that the tooth germ for tooth #23 split or divided into two since, if that tooth is counted as two, there are five incisors (five arrows), one more than expected. The geminated tooth will generally have a single root and common pulp canal. The facial view is seen in (A), and the incisal view of the same mouth is shown in (B).

FIGURE 11-12. Deep labial grooves on all four maxillary central incisor crowns and four canine roots (maxillary and mandibular) of a Native American. Notice the similarity in morphology of these wide, notched incisor crowns with the crowns of geminated teeth.
4. Fusion
Fusion is the union of two adjacent tooth germs, always involving the dentin. Upon clinical examination, this condition appears similar to gemination since the two fused teeth have one crown that appears doubled in width. However, unlike gemination, they usually reveal two separate but fused roots (seen in Fig. 11-13) with separate pulp chambers as seen on radiographs. Another way to differentiate fusion from gemination is to count the teeth in the arch. If the fused teeth are counted as two, the total number of teeth will reflect the normal number of teeth in that arch (Fig. 11-14A and B). Like geminated teeth, fused teeth occur more commonly in the anterior portion of the mouth [but in <1% of the population] and more often in the primary dentition than in the permanent dentition. The mandibular incisor area is affected more often than the maxilla.2,3 Look at the primary dentition in Figure 11-14C and determine what condition you suspect.
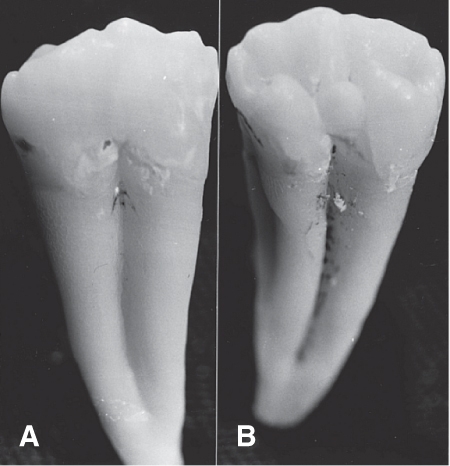
FIGURE 11-13. Fusion. Two teeth appear to be fused together. Buccal aspect (A) and lingual aspect (B). Some separation between the roots is visible. There are two pulp canals.

FIGURE 11-14. Fusion. A. If the tooth that is twice as wide as it should be is counted as two, the number of incisors is four (four arrows)—the expected number. Therefore, we suspect that the maxillary right lateral and central incisor have fused. Another possibility is the fusion of the central incisor and a supernumerary mesiodens, and the lateral incisor is congenitally absent. B. Four teeth (four arrows) appear like three crowns due to the fusion of a mandibular central and lateral incisor. C. What condition do you suspect in this mouth? Answer: Teeth N and O appear normal, but the double-wide remaining “incisor” appears to be the result of the fusion of tooth P and Q.
It is thought that fusion is caused by pressure or force during development of adjacent roots. Many of the reports of fusion involve a supernumerary tooth joining with an adjacent tooth, such as the fusion of a mandibular third and fourth molar seen in Figure 11-15A–C or the fusion of a maxillary lateral incisor and anterior supernumerary tooth.16–18

FIGURE 11-15. Fusion. A. Unusual maxillary third molar with a supernumerary paramolar fused to its distal surface. B. Paramolar fused to the buccal surface of a maxillary third molar. C. Paramolar fused to the lingual surface of a maxillary third molar.
5. Hutchinson Incisors and Mulberry Molars
When an infected mother passes syphilis on to her unborn baby, the child’s teeth in both dentitions may develop with unique shapes. Maxillary and mandibular incisors may be screwdriver shaped, broad cervically, and narrowing incisally, with a notched incisal edge. These teeth are referred to as Hutchinson incisors. Note in Figure 11-16A that the crowns of Hutchinson incisors resemble somewhat the notched crowns of fused incisors seen in Figure 11-14A and B. Also, first molars in these dentitions may have occlusal anatomy made up of multiple tiny tubercles with poorly developed indistinguishable cusps. Because of the berry-like shape on the occlusal surfaces, these molars are called mulberry molars (Fig. 11-16B). Other manifestations of congenital syphilis may include scarring of the skin around the mouth, bone pain, and swelling of the joints.

FIGURE 11-16. Two effects of congenital syphilis on the teeth. A. Hutchinson incisors are notched on these maxillary central incisors of a 9-year-old female. (Model courtesy of Dmitri J. Harampopoulos, D.D.S.) B. Each mulberry molar (at arrows) resembles the shape of a mulberry with many tubercles.
6. Accessory Cusps, Tubercles, or Ridges
Accessory enamel projections may result from developmental localized hyperplasia (increase in volume of tissue caused by growth of new cells), or crowded conditions prior to eruption may result in fusion of a supernumerary tooth, which can appear similar to an extra cusp (Fig. 11-17A–C). A third lingual cusp may develop on mandibular molars on the lingual surface and is called a tuberculum [too BER ku lum] intermedium (Fig. 11-18). If this extra cusp were located on the distal marginal ridge, it would be called a tuberculum sextum.

FIGURE 11-17. Extra cusps. A. Extra buccal cusp (or a fused paramolar) seen on the buccal surface of a maxillary second molar. B. Two extra cusps (or two fused paramolars) on the buccal surface of a maxillary molar. C. Extra buccal cusp on a mandibular molar.

FIGURE 11-18. Tuberculum intermedium (arrows). Mandibular first and second molars with extra, midlingual cusps, each called a tuberculum intermedium.
A talon cusp (like a “claw of bird of prey”) is a small projection on the lingual surface of maxillary or mandibular anterior permanent teeth (Fig. 11-19A). Frequently, the cusp has a pulp horn so that on a radiograph, it may be mistaken for a supernumerary tooth superimposed over an anterior tooth or a dens in dente (described later in this chapter). Removal of this cusp is often necessary because of its interference in jaw closure in the maximum intercuspal position. Since the pulp horn is present, endodontic treatment is usually required when this cusp is removed.2,19 The malformed marginal ridge that extends over much of the lingual surface on the anterior tooth in Figure 11-19B resembles a talon cusp.

FIGURE 11-19. Talon cusps. A. Lingual view of two maxillary central incisors with talon cusps. B. Lingual view of a maxillary left lateral incisor shows an enamel prominence in the lingual fossa that appears similar to a talon cusp. The lingual defects in all three of these teeth could affect the occlusion.
Recall that mandibular second premolars most often have three cusps (one buccal and two lingual). However, the number of lingual cusps can range from one to three, so occlusal morphology can vary greatly in terms of groove and fossa patterns established by the number of lingual cusps.20
Teeth may also exhibit extra small enamel projections called tubercles (Fig. 11-20), or extra accessory cusps. Finally, an unusual prominent ridge is seen on the facial surface of a maxillary central incisor in Figure 11-21.

FIGURE 11-20. Tubercles. A. Elevations or tubercles (or cusplets) on the cingula of a canine and lateral incisor. B. Pronounced tubercles on the cingula of maxillary anterior teeth, most noticeable (due to lighting) on the patient’s left central and lateral incisor and canine. C. Proximal views of both mandibular first premolars from a young Native American showing tubercles emanating from the triangular ridges of the buccal cusps.

FIGURE 11-21. Unusually prominent labial ridge on a secondary maxillary central incisor.
7. Variations in Tooth Size
Microdontia (very small, but normally shaped teeth) and macrodontia (very large, but normally shaped teeth) may occur as a single tooth, several teeth, or all teeth in a dentition.21 Macrodontia most frequently involves incisors and canines, whereas microdontia affects maxillary lateral incisors and third molars.11,22,23 Some examples of variation in size of teeth are shown in Figure 11-22A and B. One report described a maxillary canine 39 mm long and a maxillary first molar 31 mm long (compared to average lengths of 26.3 and 20.1 mm, respectively), both removed from a pituitary giant.21

FIGURE 11-22. Variation in tooth size from macrodontia (very large) to microdontia (very small). A. Macrodontia of two very long incisors (one 34 mm long). B. Microdontia of three very short central incisors with dwarfed roots.
8. Shovel-Shaped Maxillary Incisors
Possibly not a true anomaly, shovel-shaped incisors are a frequently occurring trait that reflect biologic differences between races.4 The lingual anatomy includes a pronounced cingulum and marginal ridges that resemble the shape of a “shovel” (Fig. 11-23A). These teeth occur most frequently in Asian, Mongoloid, Arctic, and Native American populations. Double shoveling refers to the pronounced lingual marginal ridges as well as prominent ridges on the mesial and distal portions of the labial surface as seen in Figure 11-23B.

FIGURE 11-23. A. Shovel-shaped permanent incisors from a young Native American dentition (incisal view). Note the prominent marginal ridges on the lingual surface. B. The range of prominent labial ridges on double-shovel–shaped incisors varies from labial ridges (barely discernible) on the left to more prominent labial ridges on the right.
Root malformations are normally only obvious on radiographs, although close examination of extracted teeth reveals much variation.
1. Enamel Pearls
Enamel pearls are small, round nodules of enamel with a tiny core of dentin. Since they are covered with enamel, they prevent the normal connective tissue attachment, may be felt with a probe, and, consequently, may lead to periodontal problems in this region.
They are found most frequently on the distal of third molars and near the buccal root furcation of molars24 (Fig. 11-24). On a radiograph, enamel pearls appear as small round radiopacities (i.e., areas appearing light or white on the exposed film).

FIGURE 11-24. Enamel pearls on maxillary molar roots, many located near the furcation.
2. Taurodontia
In taurodontia, or so-called bull or prism teeth, the pulp chamber is very long, without a constriction near the cementoenamel junction (Fig. 11-25). This occurs only in permanent teeth [with a frequency of less than 1 in 1000 among American Indians and some Arctic populations].25 Taurodontia is caused by a disorganization of the calcified tissues and possibly occurs in dentitions subjected to heavy use.

FIGURE 11-25. Taurodontia. Photograph of extracted tooth on left; radiographic shape outlined on right. (Courtesy of Professor Rudy Melfi, D.D.S.)
3. Dilaceration
Dilaceration [die lass er A shun] is a severe bend or angular distortion of a tooth root (Fig. 11-26).26 This unusual occurrence may be the result of a traumatic injury or of insufficient space for development, as is often the case with third molars (Fig. 11-27). Dilaceration is often observed in teeth with accessory roots. Historically, flexion is another term that has been used to describe a sharp curvature or bend of a tooth root. This condition makes it challenging to extract the tooth without breaking the root.

FIGURE 11-26. Dilaceration. A–C. Three teeth with dilaceration (or flexion) of the root.

FIGURE 11-27. Extra root and dilaceration (severe) of a mandibular molar with three instead of two roots.
4. Dens in Dente
Dens in dente [denz in DEN tee] (literally “tooth within a tooth”) is a developmental anomaly resulting from the invagination of the epithelium of the enamel organ before the formation of hard tissue (seen in Fig. 11-28A). Clinically, it appears most often as a deep crevice near the cingulum region of incisors, and on a radiograph, it appears like a tooth forming within a tooth (Fig. 11-28B). Although most commonly found in maxillary lateral incisors, this condition has also been noted in maxillary central incisors and in mandibular incisors. Usually, it appears in the coronal third of the tooth but may extend apically into the root. Often peg-shaped lateral incisors, with failure of mesial and distal lobes to develop, are found to have dens in dente upon radiographic examination. [Their occurrence is from 1% to 5% of the population.2]

FIGURE 11-28. Dens in dente (“tooth within a tooth”). A. A faciolingual, very thin cross section of a maxillary lateral incisor with a dens in dente. The defect within the tooth that connects with the lingual pit is seen here and may be an area where dental decay can occur. B. Radiograph of a dens in dente on a maxillary right central incisor. (Courtesy of Professor Rudy Melfi, D.D.S.)
5. Concrescence
Concrescence [kon KRES ens] involves the superficial fusion or growing together of only the cementum of two adjacent tooth roots (Fig. 11-29). Unlike fusion, these teeth usually become joined after eruption into the oral cavity due to the close proximity of the roots and excessive cementum deposition.6 This anomaly occurs most frequently in the maxillary molar region.

FIGURE 11-29. Concrescence is the junction or joining of cementum between adjacent teeth. Here, the cementum of a maxillary first molar is joined to the cementum of an adjacent second molar. Left: Lingual view. Right: Disto-occlusal aspect with the buccal toward the right.
6. Dwarfed Roots
Maxillary teeth often exhibit normal-sized crowns with abnormally dwarfed (short) roots (seen earlier in Fig. 11-22B). The incisal edges of maxillary teeth with dwarfed roots are often displaced lingually (as also occurs on mandibular incisors). This condition is often hereditary; however, isolated or generalized dwarfing of roots may also result from orthodontic movement of the teeth (with braces) when the movement has occurred too rapidly.
7. Hypercementosis
Hypercementosis is the formation of excess cementum around the root of a tooth after the tooth has erupted (Fig. 11-30). It may be caused by trauma, metabolic dysfunction, or periapical inflammation. Excess cementum may actually form a thin layer that connects adjacent roots, similar to the thin tissue that connects the “toes” on the webbed foot of a duck.

FIGURE 11-30. Hypercementosis or excess cementum thickness is evident on a variety of teeth.
8. Extra (Accessory) Roots
Usually occurring in teeth whose roots form after birth, accessory roots are probably caused by trauma, metabolic dysfunction, or pressure. Third molars are the multirooted teeth most likely to exhibit accessory roots (Fig. 11-31A).2 Other molars may also develop extra roots, as seen on a mandibular molars in Figure 11-31B and C. The single-rooted teeth most likely to have an extra root are the mandibular canines followed by mandibular premolars. Two roots on a mandibular canine (one facial and one lingual) are found rarely enough to be interesting but frequently enough not to be amazing (Fig. 11-32A). Mandibular first premolars may also exhibit a bifurcated root, one buccal, and one lingual (Fig. 11-32B), a condition less common for these teeth than for mandibular canines. A rare occurrence of two roots on mandibular premolars, one mesial and one distal like on mandibular molars, is evident in the radiographs in Figure 11-32C and on an extracted mandibular first premolar in Figure 11-32D. [A Japanese study of 500 mandibular first premolars found that this type of bifurcation occurred in 1.6% of Japanese teeth. These researchers also found one very rare specimen with three roots, two buccal and one lingual.27]

FIGURE 11-31. Extra roots. A. Three examples of extra (accessory) roots in a young Native American: The two larger teeth are permanent contralateral first mandibular molars, and the smaller tooth (in the center) is a primary second molar. B. Permanent mandibular left second molar with extra rootlike appendage in the furcation area. C. Two radiographs showing a right and left mandibular first molar, each with three (instead of two) roots.

FIGURE 11-32. Unusual bifurcated roots. A. Two mandibular canines with a bifurcated root (one facial and one lingual). B. Two mandibular right first premolars with bifurcated roots, a condition that is less common on this tooth than on mandibular canines. C. Radiograph showing both first and second mandibular premolars with mesial and distal roots. This mesiodistal split is quite rare. A more common occurrence is for mandibular first premolars to have their root divided buccolingually (as in B). D. A rare mandibular first premolar with a mesial and distal root.
A very unusual maxillary first premolar with three roots (two buccal and one lingual) similar to the roots of a maxillary molar is seen in Figure 11-33. There have also been a number of reports of bifurcated roots on primary maxillary canines: five discovered from routine radiographic examination and the sixth on a routine dental recall examination (as seen in Fig. 11-34).21,28–33

FIGURE 11-33. Unusual trifurcation on a maxillary premolar. Three views of a maxillary right first premolar with a normal-looking crown but with three roots: two buccal and one lingual root (mesiobuccal, distobuccal, and lingual). These roots somewhat resemble those found on maxillary molars. (A) is the mesial view, (B) is the distal view, and (C) is the occlusal view.

FIGURE 11-34. Unusual bifurcation seen on buccal views of primary maxillary canines.28 The left tooth was extracted from a 9-year-old African American child (mesial surface is to the right). The middle and right teeth came from a 5-year-old Native American child in Woods County, Ohio, believed to have lived over 2500 years old. Mesial sides face each other. (Courtesy of Dr. Ruth B. Paulson.)
C. ANOMALIES IN TOOTH POSITION
1. Unerupted (Impacted) Teeth
Unerupted teeth are embedded teeth that fail to erupt into the oral cavity because of a lack of eruptive force. Impacted teeth, on the other hand, fail to erupt due to mechanical obstruction, often related to the evolutionary decreasing size of modern man’s jaw. The most common teeth to be impacted are maxillary and mandibular third molars (Fig. 11-35A and B) and maxillary canines.2,4,34 [At least 10% of the population have impacted teeth.]

FIGURE 11-35. Impacted mandibular third molar. A. Because of its horizontal position, this third molar is mechanically locked beneath the distal bulge on the second molar and cannot erupt. B. A horizontally impacted third molar (#32) has its occlusal surface in contact with the occlusal surface of a fully formed impacted 4th molar (at arrow).
2. Misplaced Teeth (Ectopic Eruption or Transposition)
Occasionally, the cells that form a tooth (tooth buds) seem to get out of place, causing teeth to emerge in unusual locations. The most common tooth involved is the maxillary canine seen in Figure 11-36A [20 of 25 cases reported],35 followed by the mandibular canine (Fig. 11-36B). Maxillary canines can even be transposed to the central incisor region.36,37 Other abnormalities in the alignment of teeth within an arch were mentioned in Chapter 9: labioversion is when a tooth is located too far to the labial like tooth #24 in Figure 11-37A, linguoversion is when a tooth is too lingual like teeth #7 and #10 in Figure 11-37A, supraeruption when a tooth is erupted beyond the occlusal plane like tooth #1 in Figure 11-37B, and infraversion when a tooth is shorter than the occlusal plane like retained deciduous tooth K in Figure 11-37C).

FIGURE 11-36. A. Switched positions for the permanent left maxillary lateral incisor and canine (top photo has these teeth labeled with arrows on a facial view, and the bottom view has the same teeth labeled on an incisal view). B. Unusual order of teeth. Bilaterally switched mandibular canines and lateral incisors, a rare occurrence. Also note the small, retained left primary lateral incisor (tooth N).

FIGURE 11-37. A. Tooth #24 is in labioversion, #s 7 and 10 are in linguoversion. B. Tooth #1 is in supraocclusion (is extruded). C. Tooth K, a retained primary tooth, is in infraocclusion.
3. Tooth Rotation
Slight rotation of a tooth is called torsiversion like tooth # 8 in Figure 11-38A. Complete rotation, where a tooth is rotated on its axis by 180°, is a rare anomaly, most common for the maxillary second premolar (Fig. 11-38B), sometimes the maxillary incisor, first premolar, or mandibular second premolar.38

FIGURE 11-38. A. A slight rotation of this tooth #8 is called torsiversion (indicated by arrow). B. Complete rotation of a permanent maxillary second premolar with its buccal surface rotated 180° so that it is now facing the lingual (at arrow).
4. Ankylosis
Ankylosis [ang ki LO sis] may be initiated by an infection or trauma to the periodontal ligament, resulting in the loss of its periodontal ligament space so the tooth root is truly fused to the alveolar process or bone. These teeth erupt into the oral cavity but, after ankylosis, fail to reach occlusion with the opposing arch and appear shorter than adjacent teeth in its arch. Many times, ankylosis of a primary tooth occurs when the permanent successor is missing. Primary mandibular second molars most often fail to continue erupting as the jaw grows. Consequently, the ankylosed tooth will be 2 to 4 mm short of occluding with an opposing tooth (as in Fig. 11-37C).
D. ADDITIONAL TOOTH DEVELOPMENTAL MALFORMATIONS (AND DISCOLORATION)
Other tooth malformations may be related to heredity or injury during formation and therefore may affect many teeth rather than just one or two specific teeth. These conditions are not anomalies, but dental professionals should be able to distinguish them from other anomalies.
There are several terms you need to be familiar with in order to understand this section. First, the suffix “-plasia” refers to formation or development. Dysplasia is a generic term that indicates abnormal development. Dysplasia can result from too little mineral content being incorporated (hypomineralization) or too little calcium (hypocalcification) incorporated into enamel or dentin. Hypoplasia is a form of dysplasia that refers to an incomplete formation of a tissue. Dysplasia of the enamel or dentin can result from a number of factors during tooth formation, such as exposure to excessive amounts of fluoride, exposure to tetracycline antibiotics, congenital syphilis, or injury to the tooth.
1. Enamel Dysplasia
Enamel dysplasia is a term used to describe a disturbance in the enamel-forming cells (ameloblasts) during early enamel formation. Enamel dysplasia may be hereditary (as with amelogenesis imperfecta) or could result from systemic causes during early tooth formation (such as exposure to a high fever, nutritional deficiencies, or an excess amount of fluoride) or local disturbances (such as trauma or periapical infection of adjacent primary teeth). Generally, variations in color (from white to yellow and brown) or variations in morphology (such as pitting or roughened enamel) can result. Several examples of enamel disturbances are presented here.
a. Amelogenesis Imperfecta
Amelogenesis imperfecta [ah mel o JEN e sis im per FEC ta] is a hereditary disorder that affects the enamel formation of both dentitions (Fig. 11-39). (“Amelo-” refers to the ameloblasts or enamel-forming cells, and “genesis” refers to the beginning formation of these cells. The word “imperfecta” means imperfect.) The partial or complete lack of enamel results in rough yellow to brownish crowns that are susceptible to decay. This condition is rare [with an incidence in the United States of 1 in 15,000].2

FIGURE 11-39. Amelogenesis imperfecta is a hereditary disorder affecting enamel formation. (Courtesy of Carl Allen, D.D.S., M.S.D.)
b. Fluorosis
Fluorosis [floor O sis] is a condition caused during enamel formation by the ingestion of a high concentration of ingested fluoride compounds in drinking water that greatly exceeds the concentration recommended for controlling decay. The amount of fluoride compounds in some naturally occurring mineral water that causes this condition is many times greater than the one part per million that is added to drinking water to effectively reduce the prevalence of decay. These teeth can exhibit a color change from white to yellow/brown spots called mottled enamel, and if severe, the tooth enamel can undergo a morphologic change resulting in the formation of pits within the enamel (pitted enamel) (seen on erupting secondary central incisors in Fig. 11-40). Clinically, all permanent teeth may be involved depending on the length of time that the person was ingesting high levels of fluoride. These teeth are most often resistant to decay.

FIGURE 11-40. Fluorosis. This condition is most evident on the maxillary and mandibular central incisors. It is seen as white coloration or mottling of color and some pitting (on partially erupted tooth #9). (Courtesy of Carl Allen, D.D.S., M.S.D.)
c. Enamel Damage Due to High Fever
Pitted enamel on permanent teeth may result from a very high fever during early childhood due to diseases such as measles.4 Usually, the tooth crowns that are developing at the time of the fever are affected. For example, a high fever at about age 2 years and 3 months can damage the enamel forming at that time on mandibular second premolars and second molars (Fig. 11-41).

FIGURE 11-41. Enamel dysplasia (hypoplasia). This tooth damage resulted from the disruption of enamel formation on the mandibular second premolar and second molar (at arrows) at about 2 years of age when these crowns were forming. (Courtesy of Carl Allen, D.D.S., M.S.D.)
d. Focal Hypoplasia (or Hypomaturation)
Focal hypoplasia is an incomplete development of enamel seen as a localized discolored spot or deformed area on a tooth. During enamel formation, this condition may result from trauma, a local infection of an adjacent abscessed primary tooth, or some other interference in enamel matrix maturation, most likely to occur in succedaneous teeth (called a Turner hypoplasia) seen in Figure 11-42. Unlike decalcification (early decay), which can usually be seen in the cervical thirds of teeth or on occlusal surfaces of posterior teeth, this form of hypomaturation generally appears in the middle third of the smooth crown surfaces (facial and lingual surfaces). The underlying enamel may be soft making the area susceptible to decay.

FIGURE 11-42. Enamel hypoplasia (focal hypomaturation) caused by a disturbance during the formative stage of the enamel matrix. A defect on the labial surface of the maxillary central incisor (a so-called Turner hypoplasia) could be caused by an infection (abscess) on the primary central incisor that preceded it.
2. Dentin Dysplasia
Dysplasias of dentin occur twice as often as those in enamel [1 in 8000].39 Abnormal development of the dentin includes hereditary and systemic conditions as follows.
a. Dentinogenesis Imperfecta
Dentinogenesis [den ti no JEN e sis] imperfecta is a hereditary disorder that affects the dentin formation of both dentitions. Clinically, all teeth have an unesthetic light blue-gray to yellow, somewhat opalescent appearance (Fig. 11-43A), hence the term hereditary opalescent dentin. On a radiograph, there may be a partial or total absence of pulp chambers and root canals since the pulp chambers and root canals may calcify (Fig. 11-43B). These teeth may be weak because of a lack of support in the dentin, so they may be susceptible to severe attrition. [This condition occurs in only about one in every 8000 persons.]

FIGURE 11-43. Dentinogenesis imperfecta (opalescent dentin) is a hereditary disorder that affects the dentin and external appearance of all teeth. A. The teeth take on a gray or yellow opalescent appearance. B. Radiographs reveal the total or partial lack of pulp chambers and canals. (Courtesy of Carl Allen, D.D.S., M.S.D.)
b. Tetracycline Stain
When the antibiotic tetracycline is taken by a pregnant woman, an infant, or a child during the time of tooth formation and calcification, it can affect developing dentin. The result is a change in tooth color depending on the dose of the drug, to a yellow or gray-brown (Fig. 11-44). The resultant staining may be generalized in the primary dentition but may also affect some permanent teeth, depending on the age at which tetracycline was administered. Since only the teeth that are calcifying during the tetracycline therapy are stained, it is possible to confirm this condition by noting the age when tetracycline was given and comparing this to the teeth that were calcifying at that age. Some persons have erroneously blamed the staining from tetracycline antibiotic therapy during tooth formation on fluoridated community drinking water, which is beneficial for both teeth and general health.

FIGURE 11-44. Tetracycline staining in this permanent dentition resulted from the administration of tetracycline antibiotic during the time that teeth are forming. Teeth have the appearance of yellow to gray-brown horizontal bands across the crowns. (The staining on tooth #8 has been covered with a tooth-colored restorative material such as composite resin.) (Courtesy of Carl Allen, D.D.S., M.S.D.)
E. CHANGES IN TOOTH SHAPE DUE TO INJURY AFTER TOOTH ERUPTION
Reactions to injury are not really anomalies but are unique changes in tooth morphology associated with a specific cause. It is important to recognize these conditions so that their etiology (causes) can be identified and modified, when possible, to avoid the causative factor(s) that could worsen the condition.
1. Attrition
Attrition is the wearing away of enamel (and eventually dentin) due to the movement of mandibular teeth against maxillary teeth during normal function and is made worse by excessive grinding together of teeth known as bruxism. Two examples of severe attrition are shown in Figure 11-45A and B. Stress greatly increases bruxism. Attrition should be distinguished from other forms of tooth damage such as abrasion and erosion since the cause of each condition, and therefore the therapy to prevent further damage, is quite different. (Recall from the discussion on bruxism in Chapter 9 that normal tooth-to-tooth contacts per day in a healthy person without occlusal problems may be as little as 7 to 8 minutes per day during mastication of food with a force that is normally less than 33 lb. Imagine, on the other hand, the potential damage to teeth (as well as muscles and the TMJ) if a bruxer bites together for 5 hours per night at pressures exceeding 190 lb!)

FIGURE 11-45. Attrition results from prolonged bruxism or grinding of the teeth. A. These anterior teeth have been worn down almost to the level of the gingival margin. B. These permanent mandibular incisors are worn down to a level where the pulp chamber had been at one time many years previously. Note the darker circular and oval areas of exposed secondary or reparative dentin visible on the incisal ridges.
2. Abrasion
The wearing away of tooth structure by mechanical means is called abrasion. A common example of abrasion (sometimes called toothbrush abrasion) results in the loss of enamel near the cementoenamel junction of the facial surfaces of crowns, especially on premolars and canines, due to improper tooth brushing techniques (Fig. 11-46). It can be caused by using a hard bristle toothbrush, a horizontal brushing stroke, and/or a gritty dentifrice. Another contributing factor to the loss of tooth structure near the cementoenamel junction is known as abfraction [ab FRAC shun], which is the bending (flexure) of the tooth caused by heavy occlusal forces. This condition is thought to result in loss of tooth structure due to separation of enamel rods near the CEJ.

FIGURE 11-46. Abrasion (sometimes called toothbrush abrasion) is due in part to incorrect horizontal tooth brushing over areas of cementum that are exposed due to the recession of the gingiva. Flexing of the teeth during heavy occlusal forces and subsequent enamel loss (called abfraction) may contribute to and appear similar to abrasion.
Occlusal abrasion results from chewing or biting hard foods or objects or from chewing tobacco and results in flattened cusps on all posterior teeth and worn incisal edges (appearing similar to attrition). An unusual type of abrasion, caused by the use for many years of a toothpick between the maxillary central incisors, has been reported by Melfi (Dr. Rudy Melfi, personal communication circa 1983). The same type of proximal abrasion has been reported from the use of a straight pin for the same purpose over many years.
3. Erosion
Erosion is the loss of tooth structure from chemical (not mechanical) means and affects smooth and occlusal surfaces. Erosion can be the result of excessive intake or use of citric acid (like in lemons) and carbonated beverages or the result of regurgitated stomach acids (seen in bulimic individuals who habitually induce vomiting, as in the “binge and purge” syndrome).2 Erosion can also occur from an unknown cause (idiopathic). Severe erosion of the lingual enamel of all maxillary anterior teeth is evident in Figure 11-47A. Careful inspection of the tooth damage evident in the figure reveals that at least one pulp horn has been exposed on the maxillary left lateral incisor. Erosion caused by sucking on lemons between the buccal mucosa and adjacent posterior teeth is seen in Figure 11-47B.

FIGURE 11-47. Erosion. A. Severe erosion is evident on the lingual surfaces of these maxillary teeth, especially the anterior teeth. This pattern of tooth destruction is typically associated with someone with severe acid reflux or repeated regurgitation in bulimic persons. Note the exposure of one pulp chamber on tooth #10. (Courtesy of Carl Allen, D.D.S., M.S.D.) B. Erosion of facial enamel (at arrows) may be caused by holding pieces of acidic fruit like lemons next to the teeth and sucking on them for an extended period of time, a habit practiced by some persons in Southeast Asia.
Careful examination of the casts of the dentition of a 23-year-old man reveals that the mandibular left first molar (#19) closely resembles a maxillary first molar, complete with what appears to be an oblique ridge and a cusp of Carabelli (Fig. 11-48). On closer examination, the first and second mandibular premolars and first, second, and third mandibular molars on both sides also appear remarkably similar morphologically to maxillary posterior teeth. The mandibular six anterior teeth unquestionably belonged to the mandibular dentition. The occlusion of the young man’s teeth was remarkably good considering the fact that maxillary posterior teeth were occluding against practically identical maxillary teeth on both sides!
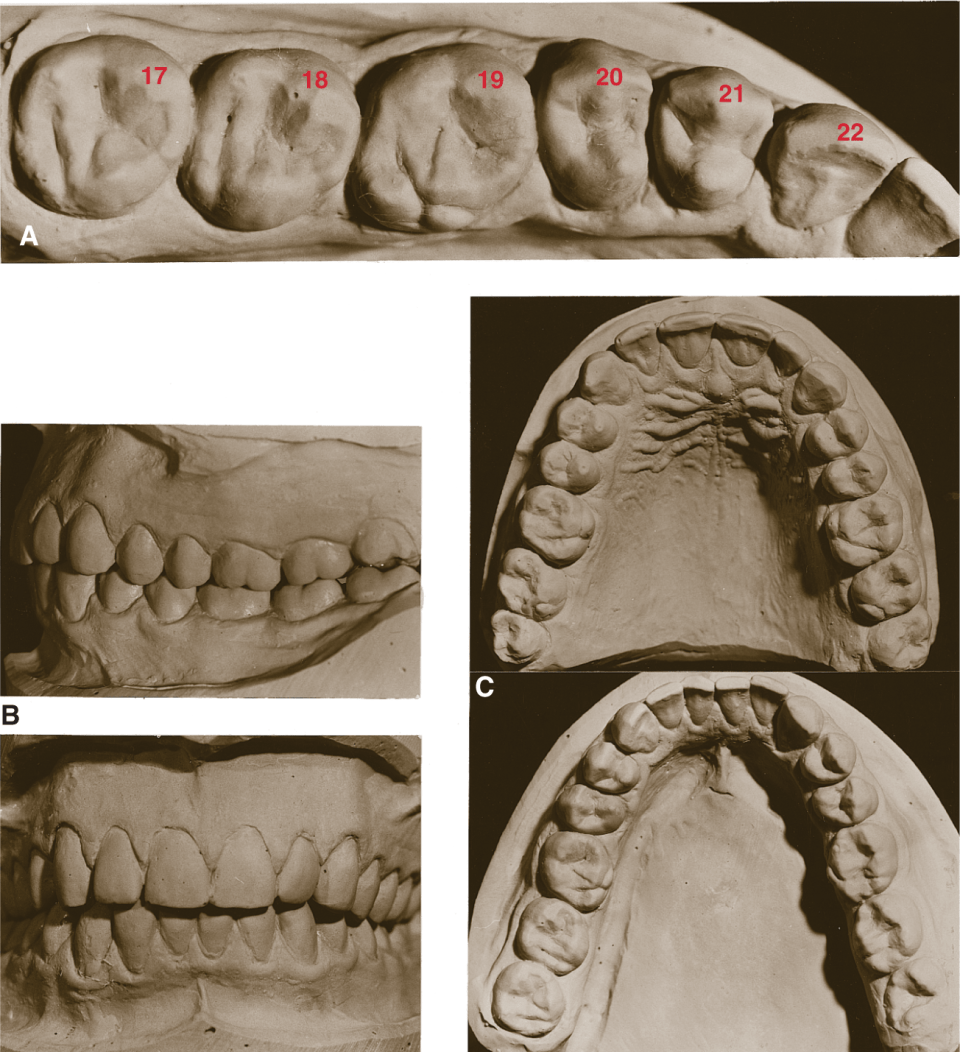
FIGURE 11-48. A most unusual mandibular dentition. A. A close-up of the mandibular dentition of a 23-year-old man who has premolars and molars with crown morphology more similar to maxillary premolars and molars, particularly on the left side. Notice that tooth #19 appears to have a cusp of Carabelli and an oblique ridge. B. The teeth as they fit together well into the maximum intercuspal position. C. Both dentitions are seen from the occlusal aspect, maxillary in the top photo and mandibular in the bottom photo. Lower premolar crowns look more like maxillary premolars. However, the six mandibular anterior teeth appear truly mandibular. The mandibular right first molar has three buccal cusps but otherwise seems to be a mixture of both maxillary and mandibular first molars: oblong mesiodistally like a lower, but with a much larger mesiolingual cusp and a Carabelli-like cusp similar to upper first molars. The mandibular left three molars seem to have only morphologic characteristics of maxillary molars. This man’s maxillary dentition seems entirely normal. It is most interesting to note that the lower left posterior teeth (particularly the premolars) have the morphology of maxillary right-side teeth. Likewise, the lower right teeth appear similar to those found in an upper left quadrant.
Another most unusual dentition of a foreign exchange student from Africa is seen in Figure 11-49. This maxillary dentition has a total of 24 erupted or partially erupted teeth. There appear to be 4 incisors, 1 canine, 6 premolars, and 13 molars (5 of which somewhat resemble mandibular molars).

FIGURE 11-49. Very unusual permanent maxillary dentition with 24 teeth, including 13 molars. This cast was furnished courtesy of J. Andrew Stevenson (D.T.L.) and Dr. Robert Stevenson, Columbus, OH.
 REVIEW Questions
REVIEW Questions
Circle the correct answer(s).
- What condition may result when a forming succedaneous tooth is located next to an abscess on an adjacent primary tooth?
- Turner hypoplasia
- Fluorosis
- Tetracycline staining
- Dentinogenesis imperfecta
- Amelogenesis imperfecta
- An adult has only three maxillary incisor crowns, but one of the crowns is doubled in width and notched. What do you suspect?
- Fusion
- Twinning
- Gemination
- Concrescence
- Cementosis
- Which condition may be caused by habitually sucking on lemons (which are quite acidic)?
- Attrition
- Erosion
- Abrasion
- Amelogenesis imperfecta
- Hypoplasia
- Which three of the following locations are most likely to have supernumerary teeth form?
- Mandibular premolar area
- Maxillary premolar area
- Maxillary incisor area
- Mandibular incisor area
- Third molar area
- Which one of the following teeth that are normally single rooted are most likely to have a bifurcated root?
- Maxillary central incisors
- Maxillary lateral incisors
- Mandibular canines
- Mandibular first premolars
- Mandibular second premolars
- Which two of the following are most likely to exhibit unusually formed crown morphology?
- Maxillary central incisors
- Maxillary lateral incisors
- Mandibular canines
- Maxillary third molars
- Maxillary first molars
ANSWERS: 1–a; 2–a; 3–b; 4–a, c, e; 5–c; 6–b, d
 CRITICAL Thinking
CRITICAL Thinking
1. List and describe as many anomalies as you can that you are likely to see in the maxillary incisor area of the mouth.
2. Search on the computer for images of “tooth anomalies” to see if you can find any other condition not already mentioned in this book.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


