Chapter 9
Rapid maxillary expansion
When the maxilla and the mandible do not ‘match’ together, it can cause a transverse malocclusion.
This occlusal problem is a discrepancy between:
- a narrow or V-shaped upper dental arch form and a U-shaped lower arch
In this case, it means that the upper buccal segment teeth are in bilateral crossbite.
In order to correct the bite, the upper jaw needs to be expanded (Figure 9.1). Rapid maxillary expansion (RME) (Figure 9.2) devices are:
- fixed-cemented onto the buccal segment teeth which incorporates a central expansion screw
The appliance:
- It works by rapidly expanding the palate, the bone of which is divided in two halves by a midline suture
- The appliance is cemented to teeth on each side
- These are joined together by an expansion screw
- The space between the two halves is initially small
- Each time the screw is turned, this space gets wider
- This can be done on patients in late mixed or second dentition up to about 15 years of age
Figure 9.1 Models of case before fitting rapid maxillary expansion.
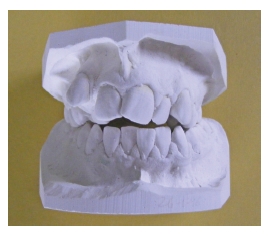
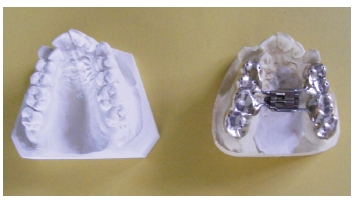
Figure 9.2 Silver casting rapid maxillary expansion appliance with model.
This has similarities to distraction osteogenesis (where the bone is surgically cut prior to expansion). The gap between the two sections of bone (in the case of the palate, the midline) must fill in and consolidate with new bone.
By turning the midline palatal screw a quarter circle turn twice daily, the upper arch widens. Patients often feel slight discomfort in the palate.
Depending on the manufacturers instructions, the number of quarter circle turns might be 40, comprising two quarter circle turns per day for 20 days.
This is followed by a passive period of 2–3 months to allow consolidation of the bone in the palate. During this time the device is left in the mouth.
When it is removed, impressions are taken and a Hawley retainer made to maintain the position achieved. This must be fitted as soon as possible to prevent relapse of the expansion.
RME devices can be made of:
- acrylic
- silver (Figure 9.3)
- soldered to bands on first permanent molars and usually pre-molars
and are made in the dental laboratory.
Unlike removable expansion appliances, they cannot be removed by the patient.
The first appointment would be for impressions.
The nurse needs to prepare:
- the patient’s clinical notes
- upper and lower impression trays
- alginate, bowl and spatula
- wax or material for bite registration
- wax knife
- method of softening wax, blow torch, flame, hot water
- bowl for gagging reflex
Figure 9.3 Silver casting rapid maxilliary expansion appliance close-up.

- tissues and mouthwash
- solution to disinfect impressions and bite
- laboratory worksheets
- plastic bags
- camera (if necessary, then also lip retractors)
and to assist the clinician at the chairside procedure, the nurse needs to:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


