Chapter 5
Caries
WHAT IS CARIES?
Caries (a Latin word meaning decay) describes the progressive destruction of enamel, dentine and cementum, initiated by microbial activity, at a susceptible tooth surface.
History and incidence
The consumption of sugar in its various forms has long been associated with the development of caries. In the United Kingdom, up until the seventeenth century, the diet consisted of unrefined whole foods, which wore occlusal surfaces flat. However, when fermentable carbohydrates became an important constituent of the Western diet in the seventeenth century, people began to develop dental caries. Also, changes in flour-milling methods, which made flour more refined, meant that less chewing was required and caries-prone fissures were not worn away. Eating patterns also began a slow, gradual change, for example, in the reign of Elizabeth I, sugar was imported and consumed by the wealthy. Dental caries became increasingly common following these changes in diet and as sugar became less expensive and more widely available to the general population.
The dental profession has been aware for over half a century that the frequency of sugar intake is far more significant in the development of caries than the amount consumed at any given time. In the present day, caries is one of the most common oral diseases found in industrialised countries, the most common cause of tooth loss in both children and adults in the Western world, and is more common in certain social classes.
According to the most recent Adult Dental Health Survey [1]:
- 24% of adults from managerial and professional occupation households had teeth with visible coronal caries (decay on crowns).
- 28% of adults from intermediate occupation households had visible coronal caries.
- 35% from routine and manual occupation households had visible coronal caries.
Although our consumption of visible sugar is declining, it is increasingly found (hidden) in many processed foods, including confectionery, soft drinks, biscuits and cakes (see Chapter 10).
It is thought that around 31% of children starting school have visible tooth decay [2]. However, the most recent UK survey [2] using the DMFT index (decayed, missing and filled teeth) also showed a gradual reduction in caries in children aged between 5 and 12 years.
This is largely due to a number of factors, including:
- Improved oral health and dietary education of parents and children.
- Wider availability and use of fluoride toothpaste.
- Regular dental check-ups identifying early problems.
In recent years, there has also been an increase in the incidence of caries in non-Western countries as diets change towards more refined sugars.
Types of caries
There are three main types of caries:
Figure 5.1 Smooth surface caries on lower molar (© Carole Hollins. Reproduced with permission)
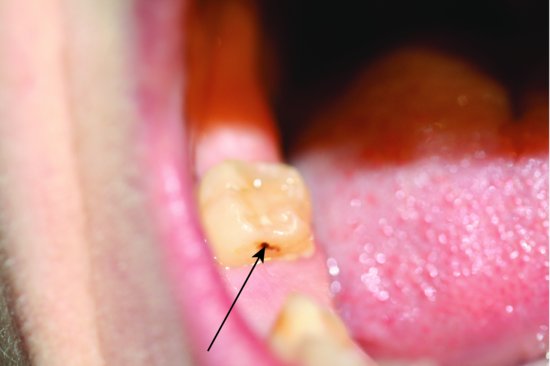
Figure 5.2 Pit and fissure caries on lower molar (© Carole Hollins. Reproduced with permission)

Figure 5.3 Root caries (© Dr Susan Hooper, Bristol University. Reproduced with permission)

Development of caries
For caries to develop, four factors are required (Figure 5.4):
Figure 5.4 Causes of caries (© Ruth McIntosh. Reproduced with permission)
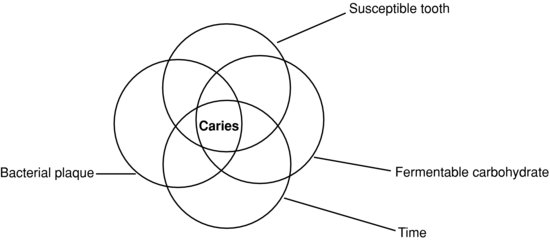
Remember! Susceptible tooth + bacterial plaque + substrate + time = caries.
Aetiology of caries
The normal (resting) pH of the mouth (and plaque) is around 6.8. This is neutral (i.e. neither acid nor alkaline).
When a susceptible tooth, often newly erupted (where the enamel has not yet matured), is exposed to frequent intakes of fermentable carbohydrates (starches that break down to sugars in the mouth), the bacteria present (most commonly
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


