3
The basics: surgical anatomy of the mandible
Placing dental implants requires access to bone tissue (usually by raising a flap) to achieve an osteotomy. The handling of soft tissues (gingiva and alveolar mucosa), and bone osteotomy must respect some anatomical structures to avoid injuries leading to damage which may be difficult to manage: reversible or irreversible nerve injury, hemorrhage, and intrusion into unwanted anatomical areas. The risk level (high, moderate, low) and the approach to prevention will be described.
ANTERIOR AREA
This region is usually considered at low risk for surgical damage. However, some anatomical structures have to be identified.
The incisive canal (Figs 3.1 and 3.2) is an anterior extension of the mandibular canal with neurovascular content. The lesion of this structure usually has no clinical consequences except in the first premolar area and sometimes in the canine area.
Figure 3.1 Mandible: mental foramen. Two anatomical variations of the inferior alveolar nerve. (A) Anterior extension: incisive canal. (B) Anterior loop. 1. Inferior alveolar nerve; 2. mental nerve; 3. incisive canal; 4. anterior loop of the inferior alveolar nerve.
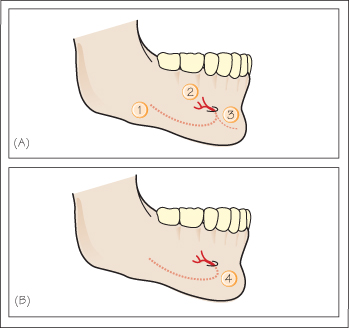
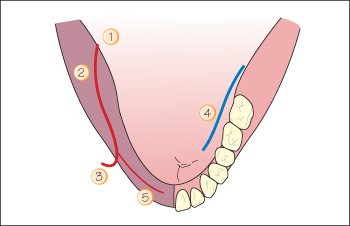
Figure 3.2 Mandible: horizontal section/occlusal view.1. Mandibular foramen; 2. mandibular canal (inferior alveolar nerve); 3. mental foramen; 4. lingual nerve; 5. incisive canal.
The lingual foramen (Fig. 3.3) can be observed on X-rays or CT scan in more than 80% of subjects near the mental spines. A branch of the sublingual artery enters the foramen to sup/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


