Chapter 25
Salivary Gland Disorders
Salivary gland disorders usually present to clinicians as enlargements (local or generalized), underactivity (xerostomia) or overactivity (ptyalism). Table 25.1 lists pathological entities by clinical classification.
Table 25.1 Pathological entities by clinical classification.
| Discrete single or multiple masses within a salivary gland |
|---|
|
| The diffusely enlarged gland |
|
Investigations
The salivary glands are easily accessible and open to a wide range of investigative techniques. The first-line investigation is often high-resolution B-mode ultrasonography. It can reliably distinguish between intra-and extraglandular masses, accurately recognize calculi/strictures and can demonstrate changes within the parenchyma. Doppler flow studies can identify vascular pathology. Conventional plain radiographs are virtually obsolete except for the ability to show small (<2 mm diameter) calculi within the ductal orifice. Traditional sialograms are still useful when investigating stones and evaluating strictures. Further evaluation can be carried out by MRI (with modest superiority over computed tomography (CT)) and recent developments such as diffusion-weighted and dynamic contrast-enhanced MRI may, in the future, permit routine visualization of the facial nerve, although at present this is still a research tool. Salivary gland scintiscans assess glandular function.
The second most useful investigation is fine-needle aspiration cytology (FNAC). The prospect of a reliable tap can be improved by ultrasound or CT-guided aspiration. A cytology service should be able to distinguish between benign and malignant disease in over 85% of cases. A correct histological diagnosis is more problematic and results cannot be relied on but the technique has particular value when a neoplasm is not suspected and if this is confirmed surgery can be avoided.
Etiology
Infection (Bacterial and Viral)
Acute Viral Sialadenitis
Over a third of all pediatric salivary gland disorders are of an inflammatory nature, with either an obstructive or non-obstructive etiology.
There is a wide range of viral infections that can involve the salivary glands (Coxsackie A and B3, parainfluenza B, ECHO type 9, and Epstein–Barr). The most common is mumps. It is caused by a highly infectious paramyxovirus with an incubation period of 2–3 weeks. The subject is infectious from 5 days prior and 10 days after the onset. In adults, the condition may be more severe and complicated by orchitis or oophoritis and varying degrees of meningoencephalitis are relatively common (25%). In rare instances, occurrence may be unilateral.
Juvenile Recurrent Parotitis
Juvenile recurrent parotitis (JRP) is a unique, non-obstructive, non-suppurative, usually unilateral variant of sialadenitis and occurs in young children. Traditionally it is considered a self-limiting condition but continual problems can occur into adult life in approximately 30–40% of cases.
It is probable there is more than one etiology: incompetent parotid ducts, juvenile Sjögren’s syndrome, lymphoma, HIV-SGD, amongst others. Congenital ductal malformations, genetic factors, bacterial or viral infection, allergy or autoimmune congenital immunoglobulin deficiency have also been postulated. The symptom-free interval may be increased following duct lavage.
Bacterial Sialadenitis
This condition is uncommon today and when it does occur it is invariably related to salivary calculi and/or a predisposing medical condition (immune suppression). It may also arise as an acute exacerbation of chronic sialadenitis. First-line treatment consists of antibiotics targeted at staphylococci and streptococci. Surgical intervention (drainage) is seldom required apart from stone removal.
Chronic/Subacute Sialadenitis
Chronic sialadenitis is usually unilateral, recurrent, and secondary to an underlying obstruction (stone or foreign body). Approximately 2% of patients with Sjögren’s syndrome are affected each year.
Autoimmune Salivary Disease
Sjögren’s Syndrome
Primary Sjögren’s syndrome has the histological features accompanied by dry eyes and mouth; if accompanied by a connective tissue disorder (systemic lupus erythematosus (SLE), polyarteritis nodosa, CREST (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia), dermatomyositis, systemic sclerosis) or primary biliary cirrhosis, it is secondary Sjögren’s. Other supposed symptom complexes have been identified (sialadenitis, nodal osteoarthritis and xerostomia, SOX). Sjögren’s syndrome subjects have a 44 times increased risk of developing lymphoma with an incidence of 5–10% of cases. It is estimated that 1% of the adult population (mean age 50 years: female predominance of 10 : 1) have Sjögren’s syndrome.
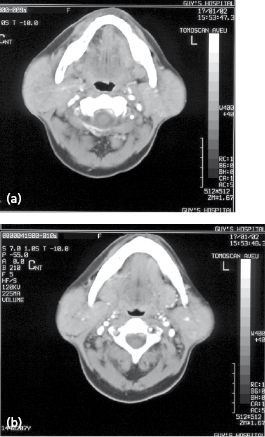
Salivary Mucosa-Associated Lymphoid Tissue (MALT) Lymphomas
These tumors are uncommon (about 1 case per million population per annum). Mikulicz (1888) described painless enlargement of the major salivary glands and lacrimal glands, which in hindsight was probably a MALT lymphoma. They are the most common lymphoma to affect salivary tissue and the third most common of the non-Hodgkin lymphomas. In the head and neck most occur in the parotid (Fig. 25.1).
Obstructive Salivary Gland Disease
In the last decade a revolution has occurred in the management of obstructive salivary gland disease with the introduction of minimally invasive techniques. Stone clearance is achieved in 80% of cases and gland removal considerably reduced. Historically the rationale for gland removal was that a calculus induces irreversible parenchyma damage, which, in turn, leads to chronic sialadenitis. There is, however, increasing evidence that salivary glands recover function following stone removal and remain asymptomatic.
Investigation
A history of repeated preprandial swelling (mealtime syndrome) is almost pathognomonic of salivary gland obstruction. Stagnant saliva leads to mucus plugs which become impacted in the stricture so symptoms typically follow a period of reduced gland activity such as sleep. The obstruction is frequently released after massage, which, in turn, is followed by a gush of salty saliva.
Ultrasonography
The main salivary glands (parotid, submandibular, and sublingual) are assessable to sonographic evaluation (frequencies of 7.5–13.5 MHz). A stone >2 mm diameter is reliably detected as an echo opaque reflection with distinct distal shadowing (Fig. 25.2). A dilated duct proximal to the echo confirms the diagnosis and dilation without an echo suggests the stricture. Consequently, ultrasound imaging can be used to monitor recovery following treatment, and portable ultrasound machines are an invaluable adjunct to current clinical practice.



