Chapter 2
Risk Factors Associated with Dental Erosion
Aim
To summarise the risk factors thought to be associated with dental erosion.
Outcome
After reading this chapter the practitioner should have an understanding of:
-
a wide range of intrinsic and extrinsic factors that increase the risk of dental erosion developing
-
the different forms of vomiting, and their aetiology, that may produce dental erosion
-
the common eating disorders that may result in dental erosion
-
the protective role of saliva
-
behaviour that increases the risk of dental erosion developing
-
the importance of a holistic and individual approach to the management of patients with dental erosion.
The Risk Factors
Exposure of the teeth to acid increases the risk of dental erosion developing. The source of the acid may be either intrinsic (from within the body) or extrinsic (from outwith the body). Extrinsic factors are wide-ranging and include dietary, environmental, medicaments’ and lifestyle agents. Figure 2-1 summarises the main risk factors.
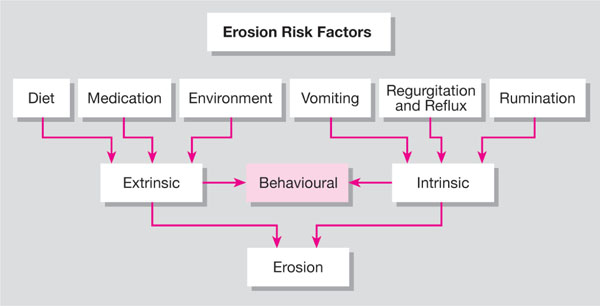
Fig 2-1 The main risk factors for erosion.
The Intrinsic Factors
Any condition or behaviour that results in acid from the gastrointestinal tract coming into contact with the teeth constitutes an intrinsic factor or a breakdown in the protective effects of saliva.
Gastric contents may reach the oral cavity in a variety of ways:
-
vomiting – the forceful expulsion of gastric contents through the mouth. The dentist should be aware that where this occurs frequently an organic or psychosomatic disorder may be the cause. These are summarised in Table 2-1.
-
regurgitation and reflux – these differ from vomiting as there is a lack of diaphragmatic muscular contraction, and a relatively small quantity of material is ejected. They are generally associated with increased gastric volume and pressure and could be a sign of an incompetent cardiac sphincter.
-
rumination – this may be considered to be a special form of regurgitation. Gastric contents are regurgitated, chewed and reswallowed. This may well be considered a variant of normal behaviour and is probably more common than reported. The social unacceptability of the practice probably inhibits disclosure.
| Causes |
Disorders of the alimentary tract
|
| Central nervous system disorders with increased intracranial pressure (e.g. encephalitis, neoplasms, hydrocephalus) |
Neurological disorders
|
Metabolic and endocrine disorders
|
Side-effect of drugs
|
Psychosomatic disorders
|
* Reproduced from Scheutzel P. Etiology of dental erosion – intrinsic factors. European Journal of Oral Sciences 1995;104:178–190, by kind permission of the Editor, Journal of Oral Sciences.
Vomiting and its variants play a significant role in a variety of eating disorders.
Eating disorders
These may be defined as a persistent disturbance of eating behaviour or behaviour intended to control weight that significantly impairs physical health or psychosocial functioning and is not secondary to a general medical condition or another psychiatric disorder. In modern western society it is believed such disorders are on the increase. Four principal types are described currently:
-
anorexia nervosa (AN)
-
bulimia nervosa (BN)
-
eating disorders not otherwise specified (EDNOS)
-
binge-eating disorder (BED)
Anorexia nervosa (AN) – although commonly believed to be a disease of the modern age, was first described independently in literature published during the 1870s by the Englishman Sir William Gull and Frenchman Ernest-Charles Lasegue. The term is derived from the greek orexis, meaning a nervous loss of appetite. It manifests as an aversion to food resulting from a complex interaction between biological, social, individual and family factors, leading to severe weight loss. Its prevalence is of the order of 0.1–1% of young females, with the average age of presentation being 16 years old. Incidence (the number of new cases in the population over one year) is estimated to be seven per 100,000. In general, affected individuals look thin and are more than 15% below ideal body weight. Two subtypes of this condition have been identified: restricting – where weight loss is accomplished primarily by either fasting or excessive exercise, or binge/purge – where loss of weight is achieved with self-induced vomiting or excessive exercise or by the misuse of laxatives, diuretics or enemas. Sufferers display a fear of gaining weight or becoming fat and have disturbed perceptions of their own body shape and size. With an obsession of self-image, there is a relentless pursuit of thinness. This is accompanied by amenorrhea and psychological disturbances.
The duration of the condition is up to six years. Significant mortality (4–20%) is associated with anorexia nervosa, given its medical complications and predisposition to suicide. The level of suicide risk is lower than with bulimia nervosa. Interestingly, a previous history of anorexia nervosa is considered to be a risk factor for the development of bulimia in later life.
Bulimia nervosa (BN) – the term is derived from the Greek bous (head of cattle) and limos (hunger) meaning literally appetite of an ox. It manifests as recurrent episodes of binge eating followed by inappropriate behaviours, such as self-induced vomiting or excessive exercise to avoid weight gain. It is a more common condition than anorexia, with a prevalence of 1–2% for adolescent girls and 0.1% for young men. Its incidence is of the order of eight to 14 cases per 100,000. The average age of presentation is 25 years. Affected individuals are less readily identifiable from their outward appearance, compared to those with anorexia nervosa, being within 10% of their physiological ideal weight. They may even be slightly overweight. Dentists may therefore be the first health professionals to detect this condition by picking up/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


